S-ar putea să vă placă și
- Anatomy & Physiology: CRH ActhDocument6 paginiAnatomy & Physiology: CRH ActhAmoroso, Marian Corneth D.Încă nu există evaluări
- Cushing SyndromeDocument12 paginiCushing SyndromeAmoroso, Marian Corneth D.Încă nu există evaluări
- Adrenal Gland DisordersDocument24 paginiAdrenal Gland Disorderssimona mariana dutuÎncă nu există evaluări
- Cushing Disease (By Syukri)Document3 paginiCushing Disease (By Syukri)Ebrahim Adel Ali AhmedÎncă nu există evaluări
- Cause/pathophysiology S&SX Interventions Listed in Priority Hypo-Adrenalism (Addison's Disease)Document5 paginiCause/pathophysiology S&SX Interventions Listed in Priority Hypo-Adrenalism (Addison's Disease)Yuka DewitzÎncă nu există evaluări
- Adrenal HyperfunctionDocument5 paginiAdrenal HyperfunctionHalla BennaaÎncă nu există evaluări
- Medical Surgical Nursing 1Document43 paginiMedical Surgical Nursing 1Tifanny Shaine Tomas100% (2)
- Med-Surg 1Document42 paginiMed-Surg 1Stephen Gabriel Tito100% (1)
- Endocrine Day 2 TemplateDocument23 paginiEndocrine Day 2 TemplateMikeÎncă nu există evaluări
- Cushing's SyndromeDocument25 paginiCushing's SyndromeRose Ann Del MundoÎncă nu există evaluări
- Adrenal Cortex - Corticosteroids Corticosteroids: GonadotrocorticoidsDocument13 paginiAdrenal Cortex - Corticosteroids Corticosteroids: GonadotrocorticoidsThierd Cañete IIIÎncă nu există evaluări
- Adrenal Gland 3: Dr. Hani Rjoob Dr. Rami AlayasaDocument34 paginiAdrenal Gland 3: Dr. Hani Rjoob Dr. Rami AlayasaMahmoud Abu MayalehÎncă nu există evaluări
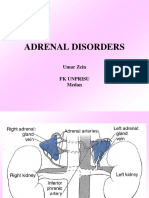
- Adrenal Disorders: Umar Zein FK Unprisu MedanDocument48 paginiAdrenal Disorders: Umar Zein FK Unprisu Medanyukmin rotamaÎncă nu există evaluări
- (MS II Lec) Endocrine System2Document8 pagini(MS II Lec) Endocrine System2IlawÎncă nu există evaluări
- Chem+Path +adrenal+2021 H+VreedeDocument39 paginiChem+Path +adrenal+2021 H+VreedeKamogelo AlbertÎncă nu există evaluări
- Cushing DiseaseDocument70 paginiCushing Diseaseاحمد المصرىÎncă nu există evaluări
- Adrenal Disorders in ChildrenDocument39 paginiAdrenal Disorders in ChildrenCorina OngÎncă nu există evaluări
- Adrenal Glands Cushing's SyndromeDocument7 paginiAdrenal Glands Cushing's SyndromeSue SongÎncă nu există evaluări
- Triads in General Surgery: Prepared by DR Narendra Allam DNB General SurgeryDocument3 paginiTriads in General Surgery: Prepared by DR Narendra Allam DNB General Surgerysk50% (2)
- Endocrine and Respiratory System DisordersDocument5 paginiEndocrine and Respiratory System Disorderssinister17Încă nu există evaluări
- Adrenal Disease VTCDocument50 paginiAdrenal Disease VTCElena Borş Morari100% (1)
- Gangguan Kel. AdrenalDocument16 paginiGangguan Kel. AdrenalInna Nur Fitri DahliyantiÎncă nu există evaluări
- Week 5 - Tutor Guide - Cushing FullDocument8 paginiWeek 5 - Tutor Guide - Cushing FullChrissitaAngelaÎncă nu există evaluări
- NCMB 316 Lecture & RleDocument34 paginiNCMB 316 Lecture & RleVenansius GanggusÎncă nu există evaluări
- Pathophysiology of CushingDocument3 paginiPathophysiology of CushingAj MacotoÎncă nu există evaluări
- Cushing Syndrom - NisaDocument17 paginiCushing Syndrom - NisaSilvanaPutriÎncă nu există evaluări
- Adrenal ColorDocument35 paginiAdrenal ColorAnonymous oOofKbmPTiÎncă nu există evaluări
- Cushing Syndrome Addisons 1Document6 paginiCushing Syndrome Addisons 1Czarena Ysabelle PayotÎncă nu există evaluări
- Adrenal Disorders: Divisi Endokrin Dan Metabolik Bagian Penyakit Dalam FK USU RSUP H. Adam Malik MedanDocument45 paginiAdrenal Disorders: Divisi Endokrin Dan Metabolik Bagian Penyakit Dalam FK USU RSUP H. Adam Malik MedanSiddiq Blackhell CakepÎncă nu există evaluări
- 005 - Cushing SyndromeDocument51 pagini005 - Cushing SyndromeLucas Victor AlmeidaÎncă nu există evaluări
- Addison+conn+cush+feo+adr IncidentalomaDocument65 paginiAddison+conn+cush+feo+adr IncidentalomaMjn BausatÎncă nu există evaluări
- Presentation Ectopic HormonesDocument12 paginiPresentation Ectopic HormonesCritic CrazzyÎncă nu există evaluări
- Week 5 - Tutor Guide - Cushing FullDocument16 paginiWeek 5 - Tutor Guide - Cushing FullChrissitaAngelaÎncă nu există evaluări
- Cushingssyndrome 180217104318Document14 paginiCushingssyndrome 180217104318Zakaria FarahÎncă nu există evaluări
- Adrenal Function: T. Creighton Mitchell, A. Wayne MeikleDocument19 paginiAdrenal Function: T. Creighton Mitchell, A. Wayne MeikleWho KnowsÎncă nu există evaluări
- Acute Liver Failure Group 3Document16 paginiAcute Liver Failure Group 31S VILLEGAS GabrielÎncă nu există evaluări
- Investigation and Management of Adrenal Disease: The Adrenal Medulla Synthesizes The Catecholamines AdrenalineDocument6 paginiInvestigation and Management of Adrenal Disease: The Adrenal Medulla Synthesizes The Catecholamines AdrenalineMarlin Berliannanda TawayÎncă nu există evaluări
- Addison's Disease FileDocument25 paginiAddison's Disease FileZyla KrisshaÎncă nu există evaluări
- 1920 Endocrine Adrenals 2Document29 pagini1920 Endocrine Adrenals 2Karl McNamaraÎncă nu există evaluări
- Diseases of The Adrenal GlandsDocument27 paginiDiseases of The Adrenal GlandsPurnima ChoudhuryÎncă nu există evaluări
- Kuliah AdrenalDocument32 paginiKuliah AdrenalNindhyana Diwaratri R100% (1)
- Renal: Cause of HTN Features Investigations PrimaryDocument9 paginiRenal: Cause of HTN Features Investigations PrimarySaadia JavaidÎncă nu există evaluări
- AdrenalDocument9 paginiAdrenalNada MuchÎncă nu există evaluări
- Adrenal InsufficiencyDocument10 paginiAdrenal InsufficiencyKhalil DiabÎncă nu există evaluări
- Cushing SyndromeDocument7 paginiCushing SyndromeFursekaÎncă nu există evaluări
- Dilantin (Phenytoin) : Drug Classification Actions Side Effects ConsiderationsDocument4 paginiDilantin (Phenytoin) : Drug Classification Actions Side Effects ConsiderationsbreehaireÎncă nu există evaluări
- Congenital Adrenal Hyperplasia: Presented By: Ahmad Fazwan JunaidiDocument16 paginiCongenital Adrenal Hyperplasia: Presented By: Ahmad Fazwan JunaidiZakirÎncă nu există evaluări
- FEARS Database-FDA Database of glp1 Disproportionate Adverse EventsDocument20 paginiFEARS Database-FDA Database of glp1 Disproportionate Adverse EventsW Antonio Rivera MartínezÎncă nu există evaluări
- Adrenal DisordersDocument48 paginiAdrenal DisordersMubeenUrRehmanÎncă nu există evaluări
- Cushing's Syndrome (Theory)Document38 paginiCushing's Syndrome (Theory)Tutde SedanaÎncă nu există evaluări
- Adrenal MassDocument38 paginiAdrenal Massshaza ewisÎncă nu există evaluări
- Adrenal Disorders: Dr. Anil Dhakal Lecturer, Internal MedicineDocument53 paginiAdrenal Disorders: Dr. Anil Dhakal Lecturer, Internal MedicineBi PinÎncă nu există evaluări
- Dr. Dwi Indria Anggraini, MSC., Spkk. Faculty of Medicine Lampung UniversityDocument36 paginiDr. Dwi Indria Anggraini, MSC., Spkk. Faculty of Medicine Lampung UniversityAnfasha_26Încă nu există evaluări
- Precipitating Factors Predisposing Factors Chronic Kidney DiseaseDocument3 paginiPrecipitating Factors Predisposing Factors Chronic Kidney DiseaseGrace Jane DionaldoÎncă nu există evaluări
- Vetcpd Adrenal Disease Notes: Sophie Keyte Bvms (Hons) Mvetmed (Dist) Dipacvim Mrcvs Sophie - Keyte@Bristol - Ac.UkDocument14 paginiVetcpd Adrenal Disease Notes: Sophie Keyte Bvms (Hons) Mvetmed (Dist) Dipacvim Mrcvs Sophie - Keyte@Bristol - Ac.UkStefana UrsuÎncă nu există evaluări
- Pitutary HeadDocument26 paginiPitutary Headdevutty 123Încă nu există evaluări
- Addison's Disease LectureDocument46 paginiAddison's Disease LectureKondwaniÎncă nu există evaluări
- Osmosis Endocrine, Pathology - Tumors - Endocrine Tumors PDFDocument7 paginiOsmosis Endocrine, Pathology - Tumors - Endocrine Tumors PDFYusril Marhaen0% (1)