S-ar putea să vă placă și
- Clin Pharm Lile Antibacterial Classes and ExamplesDocument4 paginiClin Pharm Lile Antibacterial Classes and ExamplesNicole BerryÎncă nu există evaluări
- FLUIDS and ELECTROLYTES: NEWBORN GUIDELINESDocument6 paginiFLUIDS and ELECTROLYTES: NEWBORN GUIDELINESDre Valdez100% (5)
- Hypoxic Ischemic Encephalopathy (Hie) : AlgorithmDocument11 paginiHypoxic Ischemic Encephalopathy (Hie) : AlgorithmAndreiMunteanuÎncă nu există evaluări
- Anti - Cancer Drugs 1Document80 paginiAnti - Cancer Drugs 1Rajkamal Sarma100% (1)
- Daftar Obat Sitostatika Yang Penyimpanan Dan Pemberiannya Terlindung Dari Cahaya PDFDocument1 paginăDaftar Obat Sitostatika Yang Penyimpanan Dan Pemberiannya Terlindung Dari Cahaya PDFAyahe YumnaÎncă nu există evaluări
- Multiple MyelomaDocument5 paginiMultiple Myelomaapi-647779956Încă nu există evaluări
- Malaysia-Drug Medicine Price List Kontrak - Pusat - Ubat-Ubatan - KKM - 31.05.13Document21 paginiMalaysia-Drug Medicine Price List Kontrak - Pusat - Ubat-Ubatan - KKM - 31.05.13Anuj Mairh67% (3)
- Chemo PrinciplesDocument3 paginiChemo PrinciplesSze Hui OoiÎncă nu există evaluări
- Role of Skin and Gut Microbiota in The Pathogenesis of Psoriasis, An Inflammatory Skin Disease (1-7)Document7 paginiRole of Skin and Gut Microbiota in The Pathogenesis of Psoriasis, An Inflammatory Skin Disease (1-7)Imam FhajrieÎncă nu există evaluări
- Bone Cancer Treatment RegimensDocument2 paginiBone Cancer Treatment RegimensAnne Lorraine BringasÎncă nu există evaluări
- Leukemia Treatment Regimens 7937Document3 paginiLeukemia Treatment Regimens 7937Irfan FathurrahmanÎncă nu există evaluări
- IfosfamideDocument4 paginiIfosfamideNurkholis AminÎncă nu există evaluări
- Melanoma Treatment RegimensDocument2 paginiMelanoma Treatment RegimensAndhika SeptariniÎncă nu există evaluări
- Brain Cancer Treatment Regimens (Part 1 of 5)Document5 paginiBrain Cancer Treatment Regimens (Part 1 of 5)Rubana Reaz TanaÎncă nu există evaluări
- Therapeutic Choices For The Medical Management of Feline LymphomaDocument8 paginiTherapeutic Choices For The Medical Management of Feline LymphomaFran PećnjakÎncă nu există evaluări
- Lung Cancer Treatment Regimens (Part 1 of 4)Document4 paginiLung Cancer Treatment Regimens (Part 1 of 4)Rubana Reaz TanaÎncă nu există evaluări
- Cisplatina UptoDateDocument44 paginiCisplatina UptoDateVagner CardosoÎncă nu există evaluări
- Ema-Co Gy GTDDocument4 paginiEma-Co Gy GTDTowhidulIslamÎncă nu există evaluări
- EWING SARCOMA TREATMENT REVIEWDocument7 paginiEWING SARCOMA TREATMENT REVIEWdewa gede eka yuditiraÎncă nu există evaluări
- Uterine Sarcoma - Pharmacologic Management - Cancer Therapy AdvisorDocument32 paginiUterine Sarcoma - Pharmacologic Management - Cancer Therapy AdvisorIrfan FathurrahmanÎncă nu există evaluări
- Harris Et Al (2013) - Docetaxel-Associated Palmar-Plantar Erythrodysesthesia - A Case Report and Review of The LiteratureDocument9 paginiHarris Et Al (2013) - Docetaxel-Associated Palmar-Plantar Erythrodysesthesia - A Case Report and Review of The LiteraturextraqrkyÎncă nu există evaluări
- Bladder Cancer Treatment Regimens: Clinical Trials, Chemotherapy OptionsDocument4 paginiBladder Cancer Treatment Regimens: Clinical Trials, Chemotherapy Optionsc.ramÎncă nu există evaluări
- DCEP chemotherapy regimen for R/R Multiple MyelomaDocument2 paginiDCEP chemotherapy regimen for R/R Multiple MyelomaGrazielle AlmeidaÎncă nu există evaluări
- Non-Hodgkin Lymphoma (NHL)Document11 paginiNon-Hodgkin Lymphoma (NHL)archanaÎncă nu există evaluări
- Blood 1999 Barlogie 55 65Document12 paginiBlood 1999 Barlogie 55 65Temeraire03Încă nu există evaluări
- Chemotherapy protocols for trophoblastic neoplasiaDocument3 paginiChemotherapy protocols for trophoblastic neoplasiaImam Hakim SuryonoÎncă nu există evaluări
- Study of Adverse Drug Reactions Associated With Chemotherapy of Breast CancerDocument7 paginiStudy of Adverse Drug Reactions Associated With Chemotherapy of Breast CancerInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- Endometrialcarcinoma r0416 7941Document2 paginiEndometrialcarcinoma r0416 7941crisibarra911Încă nu există evaluări
- Chemoregimen - Testicular CancerDocument2 paginiChemoregimen - Testicular CancerNanda Asyura RizkyaniÎncă nu există evaluări
- Ovarian Germ Cell Tumors Treatment EssentialsDocument7 paginiOvarian Germ Cell Tumors Treatment EssentialsMuhammad Ferhat E.S.Încă nu există evaluări
- Protocol Outline Remission Induction (6-7 Weeks)Document3 paginiProtocol Outline Remission Induction (6-7 Weeks)Mohammed HaiderÎncă nu există evaluări
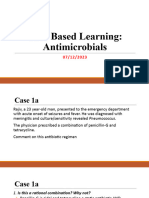
- Case Based Learning Antimicrobials 05-12-2023Document50 paginiCase Based Learning Antimicrobials 05-12-2023aditya.3757Încă nu există evaluări
- Seminar Obgyn Chemotheraphy in GynaecologyDocument38 paginiSeminar Obgyn Chemotheraphy in GynaecologyRoshandiep GillÎncă nu există evaluări
- Primary Therapy-Chronic Smoldering: ContinuedDocument2 paginiPrimary Therapy-Chronic Smoldering: ContinuedYuliana Eka RusdiyantiÎncă nu există evaluări
- Squamous Cell Cancers: Primary Systemic Therapy + Concurrent RadiotherapyDocument5 paginiSquamous Cell Cancers: Primary Systemic Therapy + Concurrent RadiotherapyArjun Singh ChoudharyÎncă nu există evaluări
- Breast Cancer RegimensDocument6 paginiBreast Cancer RegimensMohammad Arwan HamdaniÎncă nu există evaluări
- Daepoch Protocolo BccancerDocument9 paginiDaepoch Protocolo BccancerLuiz MeloÎncă nu există evaluări
- L 51 R Hypercvad R MaDocument7 paginiL 51 R Hypercvad R MaMohamed MahmoudÎncă nu există evaluări
- Doxorubicin (Conventional) : Drug Information - UpToDateDocument55 paginiDoxorubicin (Conventional) : Drug Information - UpToDateramangÎncă nu există evaluări
- Treatment Options and Side Effects for Breast CancerDocument66 paginiTreatment Options and Side Effects for Breast CancerMawin VongsaisuwonÎncă nu există evaluări
- Cetuximab-200mg Per 100ml InjectionDocument17 paginiCetuximab-200mg Per 100ml InjectionMd. Abdur RahmanÎncă nu există evaluări
- SMILEPEG HEM TCell ADocument5 paginiSMILEPEG HEM TCell Aphillip.chung89Încă nu există evaluări
- Parasite Drug of Choice 2013Document31 paginiParasite Drug of Choice 2013Ricky ImranÎncă nu există evaluări
- B-Cell Lymphomas Treatment Regimens - Follicular Lymphoma (Grade 1-2) - Cancer Therapy Advisor PDFDocument12 paginiB-Cell Lymphomas Treatment Regimens - Follicular Lymphoma (Grade 1-2) - Cancer Therapy Advisor PDFOleques Rodriguês MuahequeÎncă nu există evaluări
- 1.13 Hyper-CVAD-MA Version 2.1Document5 pagini1.13 Hyper-CVAD-MA Version 2.1Alina CrissÎncă nu există evaluări
- Uptodate Terms of Use: Author: Section Editors: Deputy EditorDocument9 paginiUptodate Terms of Use: Author: Section Editors: Deputy EditorXtineÎncă nu există evaluări
- WF10 AutoinmuneDocument11 paginiWF10 AutoinmuneFernando GarridoÎncă nu există evaluări
- Castration-Recurrent Prostate Cancer First-Line Therapy: No Visceral MetastasesDocument2 paginiCastration-Recurrent Prostate Cancer First-Line Therapy: No Visceral Metastasesalberto cabelloÎncă nu există evaluări
- Revision 1Document21 paginiRevision 1NaifmxÎncă nu există evaluări
- Improved Survival Outcome of Childhood Acute Myeloid Leukemia With Intensified Chemotherapy in Chinese ChildrenDocument12 paginiImproved Survival Outcome of Childhood Acute Myeloid Leukemia With Intensified Chemotherapy in Chinese ChildrenneizhaÎncă nu există evaluări
- Anticancer Activity of Bioactive Compounds From Kaempferia Rotunda Rhizome Against Human Breast CancerDocument8 paginiAnticancer Activity of Bioactive Compounds From Kaempferia Rotunda Rhizome Against Human Breast CancerLivia TanjungÎncă nu există evaluări
- Intensified Tuberculosis MeningitisDocument18 paginiIntensified Tuberculosis MeningitisGina ArianiÎncă nu există evaluări
- Case-Based Learning Nausea and Vomiting: Sang Ayu Putu Wahyu Pratiwi NIM. 2208612048Document8 paginiCase-Based Learning Nausea and Vomiting: Sang Ayu Putu Wahyu Pratiwi NIM. 2208612048sang ayu putu wahyu pratiwi233Încă nu există evaluări
- Anti-Tuberculosis Treatment: DR Wong VF Sibu GH 27/7/2013Document27 paginiAnti-Tuberculosis Treatment: DR Wong VF Sibu GH 27/7/2013Widy StefannyÎncă nu există evaluări
- Pelvic Ewing Sarcoma: A Retrospective Analysis of 241 CasesDocument9 paginiPelvic Ewing Sarcoma: A Retrospective Analysis of 241 CasesHassan AlmasriÎncă nu există evaluări
- Combination therapy more effective than single agents for platinum-resistant ovarian cancerDocument10 paginiCombination therapy more effective than single agents for platinum-resistant ovarian cancerJennyJessicaSÎncă nu există evaluări
- Laboratory Diagnosis: 1. Cytological Examination (Tzanck Smear)Document11 paginiLaboratory Diagnosis: 1. Cytological Examination (Tzanck Smear)Rahma P T RambeyÎncă nu există evaluări
- Jenis Obat Anti Kanker 1. Vincristine KalbeDocument5 paginiJenis Obat Anti Kanker 1. Vincristine Kalbelidya mustikaÎncă nu există evaluări
- Denosumab-12mg Per 1.7ml Single Use Vial InjectionDocument10 paginiDenosumab-12mg Per 1.7ml Single Use Vial InjectionMd. Abdur RahmanÎncă nu există evaluări
- Childhood Membranoproliferative Glomerulonephritis Type I: Limited Steroid TherapyDocument7 paginiChildhood Membranoproliferative Glomerulonephritis Type I: Limited Steroid TherapyKiki Celiana TiffanyÎncă nu există evaluări
- ADPTBDocument41 paginiADPTBHarlinda myraÎncă nu există evaluări
- pharmacoeconomics for folderDocument22 paginipharmacoeconomics for folderSurabi DevarajuÎncă nu există evaluări
- Head and Neck Cancer Chemotherapy TechniquesDocument62 paginiHead and Neck Cancer Chemotherapy Techniquesyunia chairunnisaÎncă nu există evaluări
- I.5 - Ab Necrotizing FasciitisDocument16 paginiI.5 - Ab Necrotizing FasciitisShameen KhanÎncă nu există evaluări
- Cervical Cancer ManagementDocument13 paginiCervical Cancer ManagementNailaÎncă nu există evaluări
- Cancer Textbook 4 (Cancer Treatment and Ovarian Cancer)De la EverandCancer Textbook 4 (Cancer Treatment and Ovarian Cancer)Încă nu există evaluări
- jcm-12-00453Document15 paginijcm-12-00453AndreiMunteanuÎncă nu există evaluări
- Cuti Bacterium 2019 Aid2019Document10 paginiCuti Bacterium 2019 Aid2019Vita BūdvytėÎncă nu există evaluări
- 1-s2.0-S2589909021000150-mainDocument12 pagini1-s2.0-S2589909021000150-mainAndreiMunteanuÎncă nu există evaluări
- 1546-0096-11-47Document10 pagini1546-0096-11-47AndreiMunteanuÎncă nu există evaluări
- 1-s2.0-S1877056817303389-mainDocument6 pagini1-s2.0-S1877056817303389-mainAndreiMunteanuÎncă nu există evaluări
- Rheumatic Manifestations of Inflammatory Bowel Diseases: A Study From The Middle EastDocument11 paginiRheumatic Manifestations of Inflammatory Bowel Diseases: A Study From The Middle EastAndreiMunteanuÎncă nu există evaluări
- Early Assessment of The Severity of Asphyxia in Term Newborns Using Parameters of Blood CountDocument3 paginiEarly Assessment of The Severity of Asphyxia in Term Newborns Using Parameters of Blood CountAndreiMunteanuÎncă nu există evaluări
- Hypoxic Ischemic Encephalopathy: Pathophysiology and Experimental TreatmentsDocument9 paginiHypoxic Ischemic Encephalopathy: Pathophysiology and Experimental TreatmentsAndreiMunteanuÎncă nu există evaluări
- Is Thrombocytopenia Suggestive of Organism-Specifi C Response in Neonatal Sepsis?Document5 paginiIs Thrombocytopenia Suggestive of Organism-Specifi C Response in Neonatal Sepsis?AndreiMunteanuÎncă nu există evaluări
- Clinical StudyDocument6 paginiClinical StudyAndreiMunteanuÎncă nu există evaluări
- Lucrare StintificaDocument8 paginiLucrare StintificaAndreiMunteanuÎncă nu există evaluări
- Thrombocytopenia in Late Preterm and Term Neonates After Perinatal AsphyxiaDocument10 paginiThrombocytopenia in Late Preterm and Term Neonates After Perinatal AsphyxiaTammy Utami DewiÎncă nu există evaluări
- EKA J.W. Team Bedah Saraf 42277 1,184,440,395Document56 paginiEKA J.W. Team Bedah Saraf 42277 1,184,440,395handryhuaÎncă nu există evaluări
- Price List Dan Stok 19 Jan 2024Document21 paginiPrice List Dan Stok 19 Jan 2024aadidilanÎncă nu există evaluări
- Daftar Ed Tablet Desember M-Z 2020: NO Nama Obat Jumlah Obat ED PabrikDocument6 paginiDaftar Ed Tablet Desember M-Z 2020: NO Nama Obat Jumlah Obat ED PabrikMelvy RochaLinnaÎncă nu există evaluări
- Pricelist PT. Pharmasolindo 2020 - Harga Jadi (Excl Diskon)Document2 paginiPricelist PT. Pharmasolindo 2020 - Harga Jadi (Excl Diskon)Imro FitrianiÎncă nu există evaluări
- Stock 290720Document30 paginiStock 290720Aiko Cheryl SalsabilaÎncă nu există evaluări
- STOK Tanggal 2019/10/10 NO KODE NAMADocument18 paginiSTOK Tanggal 2019/10/10 NO KODE NAMASapta RuntuweneÎncă nu există evaluări
- Daftar Kebutuhan Obat MTQDocument2 paginiDaftar Kebutuhan Obat MTQDian hariyantiÎncă nu există evaluări
- RStok Barang Dan HargaDocument45 paginiRStok Barang Dan Hargaamaliana ilmiÎncă nu există evaluări
- Precios Droexsa 13-04-2021 (Revisado)Document15 paginiPrecios Droexsa 13-04-2021 (Revisado)Laura PeñaÎncă nu există evaluări
- TUGAS KULIAH FARMASETIKA CARI NAMA SINONIM/DAGANG DAN KHASIAT OBATDocument3 paginiTUGAS KULIAH FARMASETIKA CARI NAMA SINONIM/DAGANG DAN KHASIAT OBATLuluk hasanahÎncă nu există evaluări
- Dina PabrikDocument112 paginiDina PabrikJungkook JeonÎncă nu există evaluări
- Manual Dispensing (Lengkap)Document14 paginiManual Dispensing (Lengkap)zayÎncă nu există evaluări
- Formulariun UPDATE 25 FEB 2022Document349 paginiFormulariun UPDATE 25 FEB 2022RISKA.SILVIAÎncă nu există evaluări
- Pesanan Obat Klinik Bumdes Sehat Trangkil AGUSTUS 2021: NO. Tanggal Nama Obat JumlahDocument7 paginiPesanan Obat Klinik Bumdes Sehat Trangkil AGUSTUS 2021: NO. Tanggal Nama Obat Jumlahapotek bendanÎncă nu există evaluări
- Price List September 2022Document61 paginiPrice List September 2022Ade IrawanÎncă nu există evaluări
- GHVGHDocument3 paginiGHVGHINDAH IKA SARININGRUMÎncă nu există evaluări
- Form Stok OpnameDocument5 paginiForm Stok OpnameSsagitaÎncă nu există evaluări
- Rekap Penerimaan Obat E-KatalogDocument39 paginiRekap Penerimaan Obat E-KatalogSantyÎncă nu există evaluări
- Daftar Dosis MaksimumDocument7 paginiDaftar Dosis MaksimumAldi AryantoÎncă nu există evaluări
- Pricelist Harga ObatDocument22 paginiPricelist Harga ObatNIRMALAÎncă nu există evaluări
- Golongan Nama Generik Nama Dagang Sistemik Topikal 1. AntifungiDocument7 paginiGolongan Nama Generik Nama Dagang Sistemik Topikal 1. AntifungiastriÎncă nu există evaluări
- Product List Ferron 2022 - MaximaDocument2 paginiProduct List Ferron 2022 - MaximaLukmanul HakimÎncă nu există evaluări
- Template Dan Panduan Data ObatDocument10 paginiTemplate Dan Panduan Data ObatAini SavitriÎncă nu există evaluări
- Daftar Obat Sirup Yang Tidak Menggunakan Propilen Glikol, Polietilen Glikol, Sorbitol, Dan/atau Gliserin/Gliserol (Berdasarkan Data Registrasi BPOM)Document13 paginiDaftar Obat Sirup Yang Tidak Menggunakan Propilen Glikol, Polietilen Glikol, Sorbitol, Dan/atau Gliserin/Gliserol (Berdasarkan Data Registrasi BPOM)Kpop VotingÎncă nu există evaluări
- Registered Medicine List 2014 FMHACADocument162 paginiRegistered Medicine List 2014 FMHACASindy ElfasÎncă nu există evaluări
- Precio de MedicamentosDocument6 paginiPrecio de Medicamentoscentro medico pacifico del norteÎncă nu există evaluări