S-ar putea să vă placă și
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Fundamentals of Automotive Electricity & ElectronicsDocument81 paginiFundamentals of Automotive Electricity & ElectronicsJohnny YmÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Fault Code 432 Accelerator Pedal or Lever Idle Validation Circuit - Out of CalibrationDocument10 paginiFault Code 432 Accelerator Pedal or Lever Idle Validation Circuit - Out of CalibrationAhmedmahÎncă nu există evaluări
- C20-C Serial No. From 05001 10093961 C90-C Serial No. From 05001Document26 paginiC20-C Serial No. From 05001 10093961 C90-C Serial No. From 05001ene sorinÎncă nu există evaluări
- Transient Stability Analysis of The IEEE 14-Bus Electric Power System PDFDocument10 paginiTransient Stability Analysis of The IEEE 14-Bus Electric Power System PDFc_h_v_k_rÎncă nu există evaluări
- AMI Parker Sea Recovery Booklet 2020Document18 paginiAMI Parker Sea Recovery Booklet 2020Vipuchit SirikhemapornÎncă nu există evaluări
- 1 11 FR 11 Substation Lightning ProtectionDocument12 pagini1 11 FR 11 Substation Lightning Protectionkhaldoun sami100% (1)
- DR Vito Vascular ApicdDocument32 paginiDR Vito Vascular ApicdluckyariadneeÎncă nu există evaluări
- DR LulukDocument32 paginiDR LulukluckyariadneeÎncă nu există evaluări
- Sesi 2 DR Daniel Tanubudi SPJP FIXXDocument41 paginiSesi 2 DR Daniel Tanubudi SPJP FIXXluckyariadneeÎncă nu există evaluări
- Abstract Instruction 30th ASMIHA 4Document16 paginiAbstract Instruction 30th ASMIHA 4luckyariadneeÎncă nu există evaluări
- Dr. Rony M Santoso - ACS From Diagnosis To Long Term Treatment - Focus On Oral AntiplateletDocument25 paginiDr. Rony M Santoso - ACS From Diagnosis To Long Term Treatment - Focus On Oral AntiplateletluckyariadneeÎncă nu există evaluări
- Closed Reduction, Traction, and Casting Techniques: Jason Tank, MDDocument75 paginiClosed Reduction, Traction, and Casting Techniques: Jason Tank, MDluckyariadneeÎncă nu există evaluări
- Warsava, 2000. Prox - FemurDocument63 paginiWarsava, 2000. Prox - FemurluckyariadneeÎncă nu există evaluări
- What Is A Bladder Diverticulum?Document3 paginiWhat Is A Bladder Diverticulum?luckyariadneeÎncă nu există evaluări
- Spina Bifida 2: NeuroDocument16 paginiSpina Bifida 2: NeuroluckyariadneeÎncă nu există evaluări
- Tibia-Open # MGDocument5 paginiTibia-Open # MGluckyariadneeÎncă nu există evaluări
- Tibial Non UnionsDocument9 paginiTibial Non UnionsluckyariadneeÎncă nu există evaluări
- Table Ii C C S: Secondary Control (Quasi-Centralized) SecondsDocument8 paginiTable Ii C C S: Secondary Control (Quasi-Centralized) SecondsKiahanÎncă nu există evaluări
- LTspice-model of Thermoelectric Peltier-Seebeck ElementDocument5 paginiLTspice-model of Thermoelectric Peltier-Seebeck ElementVinicius Silva OliveiraÎncă nu există evaluări
- Freesunpower - 1 Basic SystemDocument4 paginiFreesunpower - 1 Basic SystemPower EngÎncă nu există evaluări
- 11AK18 SM 30pDocument30 pagini11AK18 SM 30prumburac13Încă nu există evaluări
- Super Duper MoxonDocument8 paginiSuper Duper Moxonrus comaresÎncă nu există evaluări
- Manufacturing Quality Plan: A Raw Material Incoming InspectionDocument4 paginiManufacturing Quality Plan: A Raw Material Incoming Inspectiongulatimanish1985Încă nu există evaluări
- Review of AntennasDocument11 paginiReview of AntennasNahum SetuÎncă nu există evaluări
- Not TafelDocument19 paginiNot Tafelorang_udikÎncă nu există evaluări
- User Manual: TRIRON N SeriesDocument60 paginiUser Manual: TRIRON N SeriesIsrael FerreiraÎncă nu există evaluări
- Engine Electric StstemDocument51 paginiEngine Electric StstemnahomÎncă nu există evaluări
- IIP2-improved Frontend Receiver Using A Mismatch Compensation LNADocument8 paginiIIP2-improved Frontend Receiver Using A Mismatch Compensation LNAwrite2arshad_mÎncă nu există evaluări
- Comparison of Different Types of Generator For Wind Energy Conversion System TopologiesDocument6 paginiComparison of Different Types of Generator For Wind Energy Conversion System TopologiesCristian NietoÎncă nu există evaluări
- Bang Olufsen Beocenter 7700 (ET)Document36 paginiBang Olufsen Beocenter 7700 (ET)Minna VirtanenÎncă nu există evaluări
- AnimatronicsDocument22 paginiAnimatronicssahapriya88% (8)
- Electrical PresentationDocument54 paginiElectrical PresentationSupriyo Mehta100% (1)
- 2 Sa 1141Document3 pagini2 Sa 1141Jesus GCÎncă nu există evaluări
- SITRANS TF 7NG3136 - enDocument106 paginiSITRANS TF 7NG3136 - enDaniel RamírezÎncă nu există evaluări
- Catalogo Transformadores DONGAN USADocument108 paginiCatalogo Transformadores DONGAN USAjpousada100% (1)
- Catalogue Vacuum Circuit Breakers 3ah3 enDocument48 paginiCatalogue Vacuum Circuit Breakers 3ah3 enmrfawadÎncă nu există evaluări
- ComponentsDocument28 paginiComponentsGyan Swaroop TripathiÎncă nu există evaluări
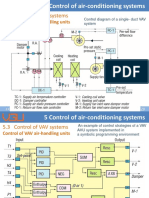
- Control of VAV Air-Handling UnitsDocument9 paginiControl of VAV Air-Handling UnitsAnh Cao Minh NgocÎncă nu există evaluări
- Aoc Le26w154Document73 paginiAoc Le26w154Ricardo EmilioÎncă nu există evaluări
- Cours Anglais 2Document7 paginiCours Anglais 2Nassim vevoÎncă nu există evaluări
- Institute Engineering Department Academic Unit-1: Discover - . EmpowerDocument34 paginiInstitute Engineering Department Academic Unit-1: Discover - . EmpowerAYUSHÎncă nu există evaluări