S-ar putea să vă placă și
- Dr. Az Rifki, Span - Kic Departemen Anestesiologi Dan Reanimasi Rsi Siti Rahmah/Fk-Fkg Universitas Baiturrahmah PadangDocument62 paginiDr. Az Rifki, Span - Kic Departemen Anestesiologi Dan Reanimasi Rsi Siti Rahmah/Fk-Fkg Universitas Baiturrahmah PadangKamelia MarcshendaÎncă nu există evaluări
- Shock: DR Terence See Consultant Emergency Department, TTSHDocument72 paginiShock: DR Terence See Consultant Emergency Department, TTSHHendri Tamara YudaÎncă nu există evaluări
- The Physiology of ShockDocument37 paginiThe Physiology of ShockGauxy AromboÎncă nu există evaluări
- Shock 19Document7 paginiShock 19Teema UmarÎncă nu există evaluări
- ShockDocument36 paginiShockJohnryan NdiranguÎncă nu există evaluări
- ShockDocument70 paginiShockDawit g/kidanÎncă nu există evaluări
- Cardiac FailureDocument63 paginiCardiac FailureNina OaipÎncă nu există evaluări
- Approach To ShockDocument30 paginiApproach To ShocktigistÎncă nu există evaluări
- Origin That Persists Beyond 24 HoursDocument3 paginiOrigin That Persists Beyond 24 Hourseric epahÎncă nu există evaluări
- Shock Study GuideDocument8 paginiShock Study GuideMadameb1Încă nu există evaluări
- ShockDocument53 paginiShockHassan Ahmed100% (3)
- ShockDocument35 paginiShocktrip100Încă nu există evaluări
- Management of Shock: DR Awoyale R.A 26th June, 2009Document78 paginiManagement of Shock: DR Awoyale R.A 26th June, 2009Ibrahim AkinbolaÎncă nu există evaluări
- Drugs Acting in CVSDocument63 paginiDrugs Acting in CVSMeghan Norico Cristuta100% (1)
- Cardiogenic ShockDocument29 paginiCardiogenic ShockagnescheruseryÎncă nu există evaluări
- EMS Shock LexDocument60 paginiEMS Shock LexIgor StefanetÎncă nu există evaluări
- Shock, Hypovolemic, AnaphylacticDocument17 paginiShock, Hypovolemic, Anaphylacticmhmdalbdyny764Încă nu există evaluări
- ShockDocument33 paginiShockVijith.V.kumarÎncă nu există evaluări
- Introduction To ShockDocument56 paginiIntroduction To ShockPaolo VegaÎncă nu există evaluări
- Pediatrics Shock DR AchuarDocument77 paginiPediatrics Shock DR AchuarShimelis TadesseÎncă nu există evaluări
- Cardiogenic Shock: by Fritzanella LafondDocument42 paginiCardiogenic Shock: by Fritzanella LafondhaphahapÎncă nu există evaluări
- Penatalaksanaan SyokDocument59 paginiPenatalaksanaan SyokArif NurfadhilahÎncă nu există evaluări
- USMLE Step 1 in Final YearDocument33 paginiUSMLE Step 1 in Final YearsehrishÎncă nu există evaluări
- 8.syncope & PresyncopeDocument11 pagini8.syncope & PresyncopeIbrahim RamizÎncă nu există evaluări
- Cardiac FailureDocument13 paginiCardiac FailureButool FatimaÎncă nu există evaluări
- .SHOCK, Alice - 1704638750000Document12 pagini.SHOCK, Alice - 1704638750000Nakintu AliceÎncă nu există evaluări
- Cardiac Tamponade: Pankaj Singh Rana Nurse Practitioner in Critical Care Swami Rama Himalayan UniversityDocument35 paginiCardiac Tamponade: Pankaj Singh Rana Nurse Practitioner in Critical Care Swami Rama Himalayan UniversityBarlonga Yhan YogaÎncă nu există evaluări
- Thea Laurene T. Tonelada BSN Iv-C Dysrhythmia: TachydysrhythmiasDocument5 paginiThea Laurene T. Tonelada BSN Iv-C Dysrhythmia: Tachydysrhythmiasscribd_lostandfoundÎncă nu există evaluări
- Shock: Anil PatidarDocument32 paginiShock: Anil Patidarjinal sutharÎncă nu există evaluări
- СердечнаяDocument70 paginiСердечнаяDaniel FunkÎncă nu există evaluări
- Hypotension & ShockDocument22 paginiHypotension & ShockEkawati ErprismanÎncă nu există evaluări
- Cardiac DysrhytmiasDocument60 paginiCardiac DysrhytmiasPY 01Încă nu există evaluări
- KP 2.5.5.4 112036 - Shock AlfanDocument52 paginiKP 2.5.5.4 112036 - Shock Alfannurul ramadhiniÎncă nu există evaluări
- Syncope: Global Cerebral Blood FlowDocument7 paginiSyncope: Global Cerebral Blood FlowChananÎncă nu există evaluări
- KGD 1 VivianDocument101 paginiKGD 1 VivianVivian SaputraÎncă nu există evaluări
- Diagnosis & Treament: ShockDocument52 paginiDiagnosis & Treament: ShockasepÎncă nu există evaluări
- Multi SistemDocument19 paginiMulti SistemciptaarynÎncă nu există evaluări
- HypertensionDocument34 paginiHypertensionmalikman80% (5)
- Shock CorrectedDocument70 paginiShock CorrectedrajevikramÎncă nu există evaluări
- 5 ShockDocument26 pagini5 Shocknightfury200313Încă nu există evaluări
- Heart FailureDocument4 paginiHeart FailureFaizan AbbasiÎncă nu există evaluări
- Lecture Presentation For Clinical 1 StudentsDocument43 paginiLecture Presentation For Clinical 1 Studentskirubel deribÎncă nu există evaluări
- Athero 2 Dr. Raquid 2021Document93 paginiAthero 2 Dr. Raquid 2021oreaÎncă nu există evaluări
- Schwartz: ShockDocument55 paginiSchwartz: ShockJovy Tan-Amodia100% (9)
- MTE Diagnosis and Manag ShockDocument52 paginiMTE Diagnosis and Manag ShockGarbha JmrsÎncă nu există evaluări
- Hypotension: Sandeep Sharma Priyanka T. BhattacharyaDocument10 paginiHypotension: Sandeep Sharma Priyanka T. Bhattacharyaمحمود محمدÎncă nu există evaluări
- Cerebrovascular DiseaseDocument20 paginiCerebrovascular DiseaseMarco GunawanÎncă nu există evaluări
- Heart Failure and ShockDocument34 paginiHeart Failure and Shockfrenee aradanasÎncă nu există evaluări
- ShockDocument49 paginiShockpaulyn ramos100% (1)
- Shock Management: by Group 7Document87 paginiShock Management: by Group 7Nur Khairah AmalinaÎncă nu există evaluări
- Cardiac Notes NursingDocument16 paginiCardiac Notes NursingYemaya8494% (17)
- Shock 2022 SeminarDocument17 paginiShock 2022 Seminarrosie100% (2)
- Assessment Cardiac SystemDocument51 paginiAssessment Cardiac Systemejarnmd100% (2)
- Prepared By: Madi, Krister: Salvador, Ma. Grace BSN-4ADocument36 paginiPrepared By: Madi, Krister: Salvador, Ma. Grace BSN-4ATap Tap100% (2)
- Shock PathophysiologyDocument63 paginiShock PathophysiologyRani OktasariÎncă nu există evaluări
- 10.15 Edrian Zulkarnain - ShockDocument42 pagini10.15 Edrian Zulkarnain - ShockBintang UbamnataÎncă nu există evaluări
- Cardio and Hema - DR PueyoDocument161 paginiCardio and Hema - DR Pueyoapi-3735995100% (2)
- ShockDocument4 paginiShockdeeÎncă nu există evaluări
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtDe la EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtEvaluare: 5 din 5 stele5/5 (1)
- Orthostatic Hypotension: Causes, Tests, and Treatment OptionsDe la EverandOrthostatic Hypotension: Causes, Tests, and Treatment OptionsÎncă nu există evaluări
- Alcohol Withdrawal Care PlanDocument1 paginăAlcohol Withdrawal Care PlanVanessaMUellerÎncă nu există evaluări
- Fluid/Electrolyte Imbalance S/S Nursing Care Fluid DeficitDocument1 paginăFluid/Electrolyte Imbalance S/S Nursing Care Fluid DeficitVanessaMUellerÎncă nu există evaluări
- Physical Assessment ChartDocument1 paginăPhysical Assessment ChartVanessaMUellerÎncă nu există evaluări
- Lab Values Chart 120511 PDFDocument5 paginiLab Values Chart 120511 PDFVanessaMUeller100% (3)
- Penuemonia Care PalnDocument2 paginiPenuemonia Care PalnVanessaMUellerÎncă nu există evaluări
- Example 1 - Focus: Nausea Related To AnestheticDocument1 paginăExample 1 - Focus: Nausea Related To AnestheticVanessaMUellerÎncă nu există evaluări
- Updated Clinical SheetDocument1 paginăUpdated Clinical SheetVanessaMUellerÎncă nu există evaluări
- Name Age Room Code Dr. Isolation Activity Diet Allergy: DX: HXDocument1 paginăName Age Room Code Dr. Isolation Activity Diet Allergy: DX: HXVanessaMUellerÎncă nu există evaluări
- Newborn Assessment NORMALDocument2 paginiNewborn Assessment NORMALVanessaMUellerÎncă nu există evaluări
- ManagmentDocument1 paginăManagmentVanessaMUellerÎncă nu există evaluări
- Admission Database PDFDocument6 paginiAdmission Database PDFVanessaMUellerÎncă nu există evaluări
- Nurse Brain Sheet Half SizeDocument1 paginăNurse Brain Sheet Half Sizevsosa624Încă nu există evaluări
- Diseases With Dermatologic ManifestationsDocument1 paginăDiseases With Dermatologic ManifestationsVanessaMUellerÎncă nu există evaluări
- Fluid/Electrolyte Imbalance S/S Nursing Care Fluid DeficitDocument1 paginăFluid/Electrolyte Imbalance S/S Nursing Care Fluid DeficitVanessaMUellerÎncă nu există evaluări
- IV PushDocument3 paginiIV PushVanessaMUeller100% (1)
- Clinical AssessementDocument2 paginiClinical AssessementVanessaMUellerÎncă nu există evaluări
- AdmimDocument2 paginiAdmimVanessaMUellerÎncă nu există evaluări
- AssessingWounds ProcedureDocument3 paginiAssessingWounds ProcedureVanessaMUellerÎncă nu există evaluări
- Alcohol Withdrawal Care PlanDocument1 paginăAlcohol Withdrawal Care PlanVanessaMUeller100% (1)
- COPD Care PLAN PDFDocument2 paginiCOPD Care PLAN PDFVanessaMUeller100% (1)
- Wound Care PDFDocument100 paginiWound Care PDFVanessaMUellerÎncă nu există evaluări
- Example 1 - Focus: Nausea Related To AnestheticDocument1 paginăExample 1 - Focus: Nausea Related To AnestheticVanessaMUellerÎncă nu există evaluări
- (Chapter 3) : Cell BiologyDocument80 pagini(Chapter 3) : Cell BiologyVanessaMUellerÎncă nu există evaluări
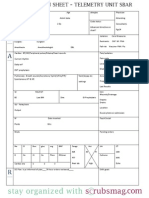
- Nurse Brain Sheet Telemetry Unit SBARDocument1 paginăNurse Brain Sheet Telemetry Unit SBARvsosa624Încă nu există evaluări
- HR Ocampo Danilo s2 E10 PDFDocument4 paginiHR Ocampo Danilo s2 E10 PDFVanessaMUellerÎncă nu există evaluări
- MedCards PDFDocument10 paginiMedCards PDFVanessaMUellerÎncă nu există evaluări
- Nurse Brain Sheet With Shift HoursDocument2 paginiNurse Brain Sheet With Shift HoursLauren Cournoyer Foreman100% (4)
- Nurse Brain Sheet Half SizeDocument1 paginăNurse Brain Sheet Half SizeRobyn GrogitskyÎncă nu există evaluări
- Wound Care PDFDocument100 paginiWound Care PDFVanessaMUeller100% (2)
- Comprehensive Head To Toe Assessment PDFDocument22 paginiComprehensive Head To Toe Assessment PDFVanessaMUellerÎncă nu există evaluări
- Prepare Active Directory and Domains For Exchange 2013 PDFDocument18 paginiPrepare Active Directory and Domains For Exchange 2013 PDFAdam DanielÎncă nu există evaluări
- Engg 135 Design of Reinforced Concrete Structures: Bond and Bar Development Reading: Wight and Macgregor Chapter 8Document24 paginiEngg 135 Design of Reinforced Concrete Structures: Bond and Bar Development Reading: Wight and Macgregor Chapter 8Manuel MirandaÎncă nu există evaluări
- Lesson10 Sacraments of InitiationDocument76 paginiLesson10 Sacraments of InitiationInsatiable CleeÎncă nu există evaluări
- Business Law Term PaperDocument19 paginiBusiness Law Term PaperDavid Adeabah OsafoÎncă nu există evaluări
- Soal Passive VoiceDocument1 paginăSoal Passive VoiceRonny RalinÎncă nu există evaluări
- Becg Unit-1Document8 paginiBecg Unit-1Bhaskaran Balamurali0% (1)
- Short StoriesDocument20 paginiShort StoriesPatrick Paul AlvaradoÎncă nu există evaluări
- Food Drug InteractionDocument23 paginiFood Drug Interactionayman_fkirin100% (5)
- I Wanted To Fly Like A ButterflyDocument12 paginiI Wanted To Fly Like A ButterflyJorge VazquezÎncă nu există evaluări
- Listen The Song and Order The LyricsDocument6 paginiListen The Song and Order The LyricsE-Eliseo Surum-iÎncă nu există evaluări
- Chapter 4Document20 paginiChapter 4Alyssa Grace CamposÎncă nu există evaluări
- Kangar 1 31/12/21Document4 paginiKangar 1 31/12/21TENGKU IRSALINA SYAHIRAH BINTI TENGKU MUHAIRI KTNÎncă nu există evaluări
- Barber ResumeDocument6 paginiBarber Resumefrebulnfg100% (1)
- PLM V6R2011x System RequirementsDocument46 paginiPLM V6R2011x System RequirementsAnthonio MJÎncă nu există evaluări
- Seafood Serving Tools Make The Task of Cleaning Seafood and Removing The Shell Much Easier. ForDocument32 paginiSeafood Serving Tools Make The Task of Cleaning Seafood and Removing The Shell Much Easier. Forivy l.sta.mariaÎncă nu există evaluări
- Burger 2005Document7 paginiBurger 2005Stefania PDÎncă nu există evaluări
- SANTHOSH RAJ DISSERTATION Presentation1Document11 paginiSANTHOSH RAJ DISSERTATION Presentation1santhosh rajÎncă nu există evaluări
- Econ 281 Chapter02Document86 paginiEcon 281 Chapter02Elon MuskÎncă nu există evaluări
- Schneider - Ch16 - Inv To CS 8eDocument33 paginiSchneider - Ch16 - Inv To CS 8ePaulo SantosÎncă nu există evaluări
- Human Rights in The Secondary SchoolDocument57 paginiHuman Rights in The Secondary SchoolJacaÎncă nu există evaluări
- Cat Enclosure IngDocument40 paginiCat Enclosure IngJuan Pablo GonzálezÎncă nu există evaluări
- Fila 1Document4 paginiFila 1Karolina Sanchez83% (6)
- Choose The Correct Answer by Crossing A, B, or C (Pilihlah Jawaban Yang Benar Dengan MemberDocument3 paginiChoose The Correct Answer by Crossing A, B, or C (Pilihlah Jawaban Yang Benar Dengan MemberJufriÎncă nu există evaluări
- Polygamy A Very Short Introduction Pearsall Sarah M S Download PDF ChapterDocument51 paginiPolygamy A Very Short Introduction Pearsall Sarah M S Download PDF Chapterharry.bailey869100% (5)
- Design and Implementation of A Computerised Stadium Management Information SystemDocument33 paginiDesign and Implementation of A Computerised Stadium Management Information SystemBabatunde Ajibola TaofeekÎncă nu există evaluări
- Essential Real AnalysisDocument459 paginiEssential Real AnalysisPranay Goswami100% (2)
- The Book of Mark: BY Dr. R. Muzira Skype: Pastorrobertmuzira Cell: 0782 833 009Document18 paginiThe Book of Mark: BY Dr. R. Muzira Skype: Pastorrobertmuzira Cell: 0782 833 009Justice MachiwanaÎncă nu există evaluări
- câu điều kiện loại 1Document5 paginicâu điều kiện loại 1ThuHoàiÎncă nu există evaluări
- Eris User ManualDocument8 paginiEris User ManualcasaleiroÎncă nu există evaluări
- Cookery Week 7 - 8 FinalDocument18 paginiCookery Week 7 - 8 FinalJay CachoÎncă nu există evaluări