S-ar putea să vă placă și
- Schierz 2016Document6 paginiSchierz 2016vivi alfiyani noorÎncă nu există evaluări
- Current Concepts and Novel Techniques in The Prosthodontic Management of Head and Neck Cancer PatientsDocument13 paginiCurrent Concepts and Novel Techniques in The Prosthodontic Management of Head and Neck Cancer Patientsvivi alfiyani noorÎncă nu există evaluări
- Program Evaluation: Presenter'S ScriptDocument3 paginiProgram Evaluation: Presenter'S Scriptvivi alfiyani noorÎncă nu există evaluări
- Marcello Machadoetal JPR2017Document9 paginiMarcello Machadoetal JPR2017vivi alfiyani noorÎncă nu există evaluări
- Journal Pone 0184041Document11 paginiJournal Pone 0184041vivi alfiyani noorÎncă nu există evaluări
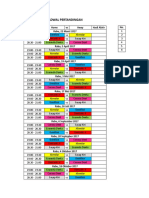
- Jadwal Pertandingan: Waktu Home Vs Away Hasil Akhir No. Rabu, 22 Maret 2017Document4 paginiJadwal Pertandingan: Waktu Home Vs Away Hasil Akhir No. Rabu, 22 Maret 2017vivi alfiyani noorÎncă nu există evaluări
- Jadwal Pertandingan: Waktu Home Vs Away Hasil Akhir No. Kamis, 23 Maret 2017Document4 paginiJadwal Pertandingan: Waktu Home Vs Away Hasil Akhir No. Kamis, 23 Maret 2017vivi alfiyani noorÎncă nu există evaluări
- Dentino Jurnal Kedokteran Gigi: Syahrial: Perbedaan Kekerasan Permukaan GigiDocument4 paginiDentino Jurnal Kedokteran Gigi: Syahrial: Perbedaan Kekerasan Permukaan Gigivivi alfiyani noorÎncă nu există evaluări
- Plaster Compound Waxes Non-Elastic Non-Elastic: Impression MaterialsDocument1 paginăPlaster Compound Waxes Non-Elastic Non-Elastic: Impression Materialsvivi alfiyani noorÎncă nu există evaluări
- Input Analisis DataDocument4 paginiInput Analisis Datavivi alfiyani noorÎncă nu există evaluări
- Ultrasonic Scaling: Associated Risks.: Review ArticleDocument5 paginiUltrasonic Scaling: Associated Risks.: Review Articlevivi alfiyani noorÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Cesars WayDocument20 paginiCesars WayToni TursićÎncă nu există evaluări
- Using The Words in The Box, Fill in All The GapsDocument23 paginiUsing The Words in The Box, Fill in All The GapsMo NoÎncă nu există evaluări
- Device InfoDocument3 paginiDevice InfoGrig TeoÎncă nu există evaluări
- High School Department PAASCU Accredited Academic Year 2017 - 2018Document6 paginiHigh School Department PAASCU Accredited Academic Year 2017 - 2018Kevin T. OnaroÎncă nu există evaluări
- Final ExamDocument2 paginiFinal ExamblacmsÎncă nu există evaluări
- This Study Resource Was: MCV4U Exam ReviewDocument9 paginiThis Study Resource Was: MCV4U Exam ReviewNathan WaltonÎncă nu există evaluări
- Resume LittletonDocument1 paginăResume Littletonapi-309466005Încă nu există evaluări
- Thermal ComfortDocument50 paginiThermal ComfortSSÎncă nu există evaluări
- LAB Find Out The Bottle ContentsDocument4 paginiLAB Find Out The Bottle ContentschanÎncă nu există evaluări
- VectorCAST QA Factsheet ENDocument2 paginiVectorCAST QA Factsheet ENChaos XiaÎncă nu există evaluări
- ArticleDocument9 paginiArticleElly SufriadiÎncă nu există evaluări
- Dr. N. Kumarappan IE (I) Council Candidate - Electrical DivisionDocument1 paginăDr. N. Kumarappan IE (I) Council Candidate - Electrical Divisionshanmugasundaram32Încă nu există evaluări
- Iso 27001 Requirementsandnetwrixfunctionalitymapping 1705578827995Document33 paginiIso 27001 Requirementsandnetwrixfunctionalitymapping 1705578827995Tassnim Ben youssefÎncă nu există evaluări
- Instructional Decision MakingDocument5 paginiInstructional Decision Makingapi-257693907Încă nu există evaluări
- VRF-SLB013-EN - 0805115 - Catalogo Ingles 2015 PDFDocument50 paginiVRF-SLB013-EN - 0805115 - Catalogo Ingles 2015 PDFJhon Lewis PinoÎncă nu există evaluări
- Contemplation (Murāqaba) and Spiritual Focus/attention (Tawajjuh) in The Pre-Mujaddidi Naqshibandi OrderDocument5 paginiContemplation (Murāqaba) and Spiritual Focus/attention (Tawajjuh) in The Pre-Mujaddidi Naqshibandi OrderShahmir ShahidÎncă nu există evaluări
- Lesson Plan Ordinal NumbersDocument5 paginiLesson Plan Ordinal Numbersapi-329663096Încă nu există evaluări
- How To Spend An Hour A Day in Prayer - Matthew 26:40-41Document1 paginăHow To Spend An Hour A Day in Prayer - Matthew 26:40-41Steve GainesÎncă nu există evaluări
- Month Puzzle Two VariableDocument6 paginiMonth Puzzle Two VariableNayan KaithwasÎncă nu există evaluări
- Topic 4 Statistic II (Form 3)Document2 paginiTopic 4 Statistic II (Form 3)Ct KursiahÎncă nu există evaluări
- Packing List For GermanyDocument2 paginiPacking List For GermanyarjungangadharÎncă nu există evaluări
- SafetyStock OverviewDocument3 paginiSafetyStock OverviewJosue FonsecaÎncă nu există evaluări
- Cascade Configuration Tool: Installation and Operations ManualDocument22 paginiCascade Configuration Tool: Installation and Operations ManualAndrés GarciaÎncă nu există evaluări
- MAPEH-Arts: Quarter 3 - Module 2Document24 paginiMAPEH-Arts: Quarter 3 - Module 2Girlie Oguan LovendinoÎncă nu există evaluări
- Citadel Securities Australia Pty LTD - Company DetailsDocument5 paginiCitadel Securities Australia Pty LTD - Company DetailsBrendan OswaldÎncă nu există evaluări
- Soal PTS Vii BigDocument6 paginiSoal PTS Vii Bigdimas awe100% (1)
- History of The Hadith, Dr. Muhammad HameedullahDocument0 paginiHistory of The Hadith, Dr. Muhammad HameedullahAMEEN AKBAR100% (4)
- Happiest Refugee Coursework 2013Document10 paginiHappiest Refugee Coursework 2013malcrowe100% (2)
- ISA Guidelines PPF 1Document19 paginiISA Guidelines PPF 1Vasu DevanÎncă nu există evaluări
- The Names of Allah and Their ReflectionsDocument98 paginiThe Names of Allah and Their ReflectionsSuleyman HldÎncă nu există evaluări