S-ar putea să vă placă și
- Oral Surgery Question BankDocument1 paginăOral Surgery Question BankBHARGAVI V MADYALKARÎncă nu există evaluări
- Atlas of Intraoperative Transesophageal EchocardiographyDocument416 paginiAtlas of Intraoperative Transesophageal EchocardiographyDelia Acsinte100% (1)
- Temporary Anchorage Device (TAD's)Document121 paginiTemporary Anchorage Device (TAD's)Chandra Sekhar Reddy100% (1)
- Biomechanics in Orthodontics - NandaDocument16 paginiBiomechanics in Orthodontics - NandaVerônica Polo Perez100% (2)
- Management of Impacted TeethDocument153 paginiManagement of Impacted TeethToma Irina100% (1)
- Fractures of The Middle Third of The Facial SkeletonDocument7 paginiFractures of The Middle Third of The Facial SkeletonMahendra Perumal50% (2)
- Mandibular Growth Rotation (2) / Orthodontic Courses by Indian Dental AcademyDocument28 paginiMandibular Growth Rotation (2) / Orthodontic Courses by Indian Dental Academyindian dental academyÎncă nu există evaluări
- Optimal Vs Ideal OcclusionDocument6 paginiOptimal Vs Ideal OcclusionshraddhaÎncă nu există evaluări
- Thesis PDFDocument98 paginiThesis PDFDr sneha HoshingÎncă nu există evaluări
- Biology of Tooth MovementDocument84 paginiBiology of Tooth Movementسلمى صلاحÎncă nu există evaluări
- Laparoscopic CholecystectomyDocument41 paginiLaparoscopic CholecystectomyLim MelaniÎncă nu există evaluări
- Orthognathic Surgery Seminar 6 FinalDocument83 paginiOrthognathic Surgery Seminar 6 FinalNikhil SrivastavaÎncă nu există evaluări
- 10.2 Major Surgical ProceduresDocument22 pagini10.2 Major Surgical ProceduresishtiiiÎncă nu există evaluări
- Occlusion, Malocclusion and Method of Measurements - An OverviewDocument7 paginiOcclusion, Malocclusion and Method of Measurements - An OverviewDiana BernardÎncă nu există evaluări
- Subbrow Blepharoplasty For Upper Eyelid Rejuvenation in AsiansDocument5 paginiSubbrow Blepharoplasty For Upper Eyelid Rejuvenation in AsiansdoctorbanÎncă nu există evaluări
- Micro Implants in OrthodonticsDocument3 paginiMicro Implants in OrthodonticsCrețu VasileÎncă nu există evaluări
- Treatment Planning Single Maxillary Anterior Implants for DentistsDe la EverandTreatment Planning Single Maxillary Anterior Implants for DentistsÎncă nu există evaluări
- Muscle Physiology / Orthodontic Courses by Indian Dental AcademyDocument93 paginiMuscle Physiology / Orthodontic Courses by Indian Dental Academyindian dental academyÎncă nu există evaluări
- Bedrossian Zygomatic Rescue PDFDocument33 paginiBedrossian Zygomatic Rescue PDFJulieÎncă nu există evaluări
- Prostho Rehabilitation - HypodontiaDocument24 paginiProstho Rehabilitation - HypodontiaAmniAzmiÎncă nu există evaluări
- Smile Analysis: Staff Incharge Dr. A. SrikanthDocument124 paginiSmile Analysis: Staff Incharge Dr. A. SrikanthLikhitaÎncă nu există evaluări
- All On Four Implant ReviewDocument12 paginiAll On Four Implant ReviewPreeti TaraiyaÎncă nu există evaluări
- Biology of Orthodontic Tooth MovementDocument16 paginiBiology of Orthodontic Tooth MovementGowri ShankarÎncă nu există evaluări
- Growth of MaxillaDocument110 paginiGrowth of Maxillaprincygarg008Încă nu există evaluări
- TMJ Postgraduate ProgramDocument8 paginiTMJ Postgraduate ProgramsorcÎncă nu există evaluări
- Concepts of Arrangement of Artifical Teeth, SelectiveDocument7 paginiConcepts of Arrangement of Artifical Teeth, SelectiveAmar BhochhibhoyaÎncă nu există evaluări
- Alveolar Bone GraftingDocument13 paginiAlveolar Bone GraftingDayal SharanÎncă nu există evaluări
- Umbilical HerniasDocument10 paginiUmbilical HerniasDiana Jane LauretaÎncă nu există evaluări
- Orthognathic Surgery RonalDocument56 paginiOrthognathic Surgery Ronaldrghempik100% (2)
- Craniofacial BookDocument111 paginiCraniofacial BookAnonymous 8hVpaQdCtr100% (1)
- Combination SyndromeDocument3 paginiCombination SyndromeNandya ZhafirahÎncă nu există evaluări
- Skeletal Anchorage in OrthodonticsDocument8 paginiSkeletal Anchorage in OrthodonticsNingombam Robinson SinghÎncă nu există evaluări
- CephalometricsDocument25 paginiCephalometricsMoola Bharath Reddy100% (2)
- Maxillofacial ProsthodonticsDocument12 paginiMaxillofacial ProsthodonticsManjeev GuragainÎncă nu există evaluări
- Criteria Optimum Functional OcclusionDocument48 paginiCriteria Optimum Functional OcclusionMako J CanadianoÎncă nu există evaluări
- TMD & Its Role in Orthodontics "TMD An Entity Affecting Every Aspect of Life" A ReviewDocument6 paginiTMD & Its Role in Orthodontics "TMD An Entity Affecting Every Aspect of Life" A ReviewInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- Interceptive Orthodontics: A Practical Guide to Occlusal ManagementDe la EverandInterceptive Orthodontics: A Practical Guide to Occlusal ManagementÎncă nu există evaluări
- Horizontal Alveolar Ridge Augmentation in Implant Dentistry: A Surgical ManualDe la EverandHorizontal Alveolar Ridge Augmentation in Implant Dentistry: A Surgical ManualEvaluare: 4.5 din 5 stele4.5/5 (2)
- TMJ OclusionDocument23 paginiTMJ OclusionMara IoanaÎncă nu există evaluări
- Soft Tissue Analysis (Autosaved)Document126 paginiSoft Tissue Analysis (Autosaved)Ayushi Toley100% (1)
- Starting An Intravenous InfusionDocument2 paginiStarting An Intravenous InfusionAmiel Francisco Reyes100% (1)
- Assisting The Patient During The Lumbar Puncture DefinitionDocument3 paginiAssisting The Patient During The Lumbar Puncture DefinitionSHAINA CADALINÎncă nu există evaluări
- FacemaskDocument30 paginiFacemaskAnushree RathiÎncă nu există evaluări
- The Osteoperiosteal Flap: A Simplified Approach to Alveolar Bone ReconstructionDe la EverandThe Osteoperiosteal Flap: A Simplified Approach to Alveolar Bone ReconstructionEvaluare: 4 din 5 stele4/5 (1)
- Ortho Perio NewDocument5 paginiOrtho Perio NewNingombam Robinson SinghÎncă nu există evaluări
- Socket PreservationDocument24 paginiSocket PreservationFadly RasyidÎncă nu există evaluări
- Krok 2 - 2021 - 26 JulyDocument19 paginiKrok 2 - 2021 - 26 JulyNicole VinnikÎncă nu există evaluări
- Classification For Zygomatic Implant PatientsDocument7 paginiClassification For Zygomatic Implant PatientsDrVarun Menon50% (2)
- Pulp Therapy For Primary TeethDocument14 paginiPulp Therapy For Primary TeethMahmoudFayedÎncă nu există evaluări
- Past Question NursingDocument37 paginiPast Question NursingOpeyemi Omolabake67% (3)
- Microsurgery in PeriodontologyDocument5 paginiMicrosurgery in PeriodontologySilviu TipleaÎncă nu există evaluări
- Oral Surgery FlapsDocument13 paginiOral Surgery Flapshaneefmdf100% (1)
- Retention and RelapseDocument92 paginiRetention and RelapseBimalKrishna100% (1)
- Clinical Maxillary Sinus Elevation SurgeryDe la EverandClinical Maxillary Sinus Elevation SurgeryDaniel W. K. KaoÎncă nu există evaluări
- Laryngeal Electromyography Emg Lemg PDFDocument3 paginiLaryngeal Electromyography Emg Lemg PDFSuprit Sn50% (2)
- Periodontal Regeneration (Lecture) 2017 PDFDocument103 paginiPeriodontal Regeneration (Lecture) 2017 PDFAhmad AliÎncă nu există evaluări
- Wilmes. and Ludwig - Mini-Implants in The Anterior PalateDocument64 paginiWilmes. and Ludwig - Mini-Implants in The Anterior Palateromulodent100% (1)
- Bone Grafting Techniques for Maxillary ImplantsDe la EverandBone Grafting Techniques for Maxillary ImplantsÎncă nu există evaluări
- Orthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentDe la EverandOrthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentFederico BrugnamiÎncă nu există evaluări
- Common Sense MechanicsDocument9 paginiCommon Sense MechanicsKarina LehnertÎncă nu există evaluări
- Orthognathic Surgery Oral SurgeryDocument24 paginiOrthognathic Surgery Oral SurgeryFourthMolar.comÎncă nu există evaluări
- Thick vs. Thin Gingival Biotypes: A Key Determinant in Treatment Planning For Dental ImplantsDocument6 paginiThick vs. Thin Gingival Biotypes: A Key Determinant in Treatment Planning For Dental ImplantsLuiz Guilherme Loivos100% (1)
- Inverted L OsteotomyDocument9 paginiInverted L OsteotomyhaneefmdfÎncă nu există evaluări
- Trauma From Occlusion PerioDocument27 paginiTrauma From Occlusion PerioFourthMolar.com100% (3)
- Tooth Eruption TheoriesDocument9 paginiTooth Eruption Theoriesindian dental academyÎncă nu există evaluări
- Anterior Open BiteDocument7 paginiAnterior Open BiteGowriÎncă nu există evaluări
- Wolff's LawDocument3 paginiWolff's Lawdrgayen6042Încă nu există evaluări
- Rapid Maxillary Expansion and ApplianceDocument4 paginiRapid Maxillary Expansion and Appliancedrzana78Încă nu există evaluări
- Cleft Lip and Palate Indices: A Review: Anju Agrawal, Rabindra Man Shrestha and Praveen MishraDocument9 paginiCleft Lip and Palate Indices: A Review: Anju Agrawal, Rabindra Man Shrestha and Praveen MishranomanÎncă nu există evaluări
- NICU Booklet April2020Document90 paginiNICU Booklet April2020Popescu VioricaÎncă nu există evaluări
- Development of Hemorrhoids: Anal Canal AnatomyDocument20 paginiDevelopment of Hemorrhoids: Anal Canal AnatomyKris TejereroÎncă nu există evaluări
- 03 In-Office Endoscopic Laryngeal Laser ProceduresDocument7 pagini03 In-Office Endoscopic Laryngeal Laser ProceduresG WÎncă nu există evaluări
- Laparaskopi HTDocument167 paginiLaparaskopi HTbarsitom100% (1)
- Intracranial Pressure (Icp)Document41 paginiIntracranial Pressure (Icp)Roadtogot 2023Încă nu există evaluări
- Maret 2018 26-50Document10 paginiMaret 2018 26-50daniel_alexander_susenoÎncă nu există evaluări
- 11.sudden Natural Death 3Document55 pagini11.sudden Natural Death 3Hasabo AwadÎncă nu există evaluări
- Esgena CDC Endos PDFDocument30 paginiEsgena CDC Endos PDFErfandi ZeinÎncă nu există evaluări
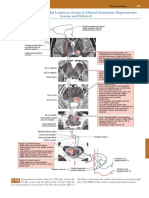
- Posterior Column-Medial Lemniscus System in Clinical Orientation: Representative Lesions and DeficitsDocument1 paginăPosterior Column-Medial Lemniscus System in Clinical Orientation: Representative Lesions and DeficitsEduardo RodriguezÎncă nu există evaluări
- Inguinal HernioplastyDocument10 paginiInguinal HernioplastyfiansisÎncă nu există evaluări
- Course f2f Inp CPRDocument9 paginiCourse f2f Inp CPRMichelle Gliselle Guinto MallareÎncă nu există evaluări
- Benign Tumors of UterusDocument44 paginiBenign Tumors of UterusZunaira ZahraÎncă nu există evaluări
- 9 IABP and Plasmapheresis (4 Files Merged)Document48 pagini9 IABP and Plasmapheresis (4 Files Merged)Alaa OmarÎncă nu există evaluări
- Juno Tech Sheet-Flyer v5Document2 paginiJuno Tech Sheet-Flyer v5Divina BlancoÎncă nu există evaluări
- L02024 Rev G Tapered Family Catalog & ManualDocument32 paginiL02024 Rev G Tapered Family Catalog & ManualDani NarváezÎncă nu există evaluări
- Clavicle: Fracture While Falling in Outstreched and Lateral 1/3Document9 paginiClavicle: Fracture While Falling in Outstreched and Lateral 1/3hyyjÎncă nu există evaluări
- Stainless Steel CrownsDocument19 paginiStainless Steel CrownsSameerChoudharyÎncă nu există evaluări
- Induction of Labor Algorithm: Appendix RDocument1 paginăInduction of Labor Algorithm: Appendix RBrolie BarsebaÎncă nu există evaluări
- Vaginal Birth After Caesarean Section (VBAC) 5.0Document21 paginiVaginal Birth After Caesarean Section (VBAC) 5.0Savira ChoiÎncă nu există evaluări
- L.P On Lambar PunctureDocument16 paginiL.P On Lambar PunctureMary MenuÎncă nu există evaluări