S-ar putea să vă placă și
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- HAYDUKE, George - ''Make'Em Pay - Ultimate Revenge Techniques From The Master Trickster''Document125 paginiHAYDUKE, George - ''Make'Em Pay - Ultimate Revenge Techniques From The Master Trickster''Mitko Krumov100% (3)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Dragonix - DM Options, Monster Talents IIDocument246 paginiDragonix - DM Options, Monster Talents IIJolticsy Rules100% (8)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- O Level Biology NotesDocument547 paginiO Level Biology NotesSsonko Edrine100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Present Perfect - Past Simple - Extensive PracticeDocument13 paginiPresent Perfect - Past Simple - Extensive PracticeDan TeÎncă nu există evaluări
- Sitting Fox: Materials KeyDocument7 paginiSitting Fox: Materials KeyVerónica TÎncă nu există evaluări
- Question Report 2478Document11 paginiQuestion Report 2478Raghav gupta100% (1)
- Science of The Heart Vol 2Document118 paginiScience of The Heart Vol 2karinadaparia75% (4)
- Interpretation Chest X RayDocument127 paginiInterpretation Chest X RayVimal NishadÎncă nu există evaluări
- Acorn Pattern.: Skills RequiredDocument5 paginiAcorn Pattern.: Skills RequiredCanela Folguerona100% (2)
- Occluion ConceptsDocument15 paginiOccluion ConceptsImran CassimÎncă nu există evaluări
- "New Welfarism, Veganism, and Capitalism," From Animal Oppression and Human Violence, by David A. NibertDocument14 pagini"New Welfarism, Veganism, and Capitalism," From Animal Oppression and Human Violence, by David A. NibertColumbia University PressÎncă nu există evaluări
- Cave PaintingsDocument9 paginiCave Paintingsabhishek behera100% (1)
- Maxillofacial Materials: Review ArticleDocument4 paginiMaxillofacial Materials: Review ArticleAli Faraz SiddiquiÎncă nu există evaluări
- Corona VirusDocument7 paginiCorona VirusMaria CorenaÎncă nu există evaluări
- Covid19 Screening QuestionnaireDocument1 paginăCovid19 Screening QuestionnaireAli Faraz SiddiquiÎncă nu există evaluări
- Assessment of A True Emergency: (Circle Patient's Response Wherever Appropriate)Document1 paginăAssessment of A True Emergency: (Circle Patient's Response Wherever Appropriate)Ali Faraz SiddiquiÎncă nu există evaluări
- IDA Recommendations For Dental Professionals On The Coronavirus ThreatDocument5 paginiIDA Recommendations For Dental Professionals On The Coronavirus ThreatAli Faraz SiddiquiÎncă nu există evaluări
- 5-11 PrashanthDocument7 pagini5-11 PrashanthMV PratyushaÎncă nu există evaluări
- Thermacol PDFDocument4 paginiThermacol PDFAli Faraz SiddiquiÎncă nu există evaluări
- Shanahan TEJ (1956)Document7 paginiShanahan TEJ (1956)Ali Faraz SiddiquiÎncă nu există evaluări
- Assignment Topic P1Document2 paginiAssignment Topic P1Ali Faraz SiddiquiÎncă nu există evaluări
- Geriatric Care Managers: Care of The Elderly Long Term Care Quality of Life Old Age ReferringDocument2 paginiGeriatric Care Managers: Care of The Elderly Long Term Care Quality of Life Old Age ReferringAli Faraz SiddiquiÎncă nu există evaluări
- Case 1 LaminatesDocument2 paginiCase 1 LaminatesAli Faraz SiddiquiÎncă nu există evaluări
- Pyott JE. and Schaeffer A (1954)Document7 paginiPyott JE. and Schaeffer A (1954)Ali Faraz SiddiquiÎncă nu există evaluări
- Saliva and Its Prosthodontic ImplicationsDocument3 paginiSaliva and Its Prosthodontic Implicationsdrvivek reddyÎncă nu există evaluări
- Arstad T (1956)Document8 paginiArstad T (1956)Ali Faraz SiddiquiÎncă nu există evaluări
- Atwood DA (1955)Document16 paginiAtwood DA (1955)Ali Faraz SiddiquiÎncă nu există evaluări
- Cohen S (1957)Document6 paginiCohen S (1957)Ali Faraz SiddiquiÎncă nu există evaluări
- 8Document5 pagini8Ali Faraz SiddiquiÎncă nu există evaluări
- Types of Reproduction: Sexual AsexualDocument45 paginiTypes of Reproduction: Sexual AsexualasdÎncă nu există evaluări
- Anatomy of The Head and The Neck FinalDocument156 paginiAnatomy of The Head and The Neck FinalYudhi Aulia100% (1)
- Reading SMPDocument43 paginiReading SMPSharah RahmawatiÎncă nu există evaluări
- Dairy India 2007Document4 paginiDairy India 2007Rama Kr M100% (1)
- Wildlife Rehabilitator License ApplicationDocument1 paginăWildlife Rehabilitator License ApplicationDaveÎncă nu există evaluări
- Tuberculosis: What Is It and How Do We Keep Healthy?: A Presentation For Pacific Island Schools and CommunitiesDocument17 paginiTuberculosis: What Is It and How Do We Keep Healthy?: A Presentation For Pacific Island Schools and CommunitiesKailash NagarÎncă nu există evaluări
- 4ES0 02 Que 20110617Document8 pagini4ES0 02 Que 20110617Syed AhadÎncă nu există evaluări
- Descriptive EssayDocument10 paginiDescriptive EssayAmhyr De Mesa Dimapilis100% (1)
- Food and Man 1Document25 paginiFood and Man 1Rejoice Gumboc MabilogÎncă nu există evaluări
- Axolotl Zoology Creative FinalDocument2 paginiAxolotl Zoology Creative Finalapi-643479863Încă nu există evaluări
- Jurnal Katak PDFDocument5 paginiJurnal Katak PDF31122007Încă nu există evaluări
- Demon Star orDocument3 paginiDemon Star orFelmerPolancoRodaÎncă nu există evaluări
- Factors Associated With Menstrual Cycle Irregularity and MenopauseDocument11 paginiFactors Associated With Menstrual Cycle Irregularity and MenopauseRyan IlhamÎncă nu există evaluări
- Published-Pdf-327-6-10. IJZAB ID No. 327 PDFDocument6 paginiPublished-Pdf-327-6-10. IJZAB ID No. 327 PDFIJZABÎncă nu există evaluări
- Chinese Vocabulary AnimalsDocument4 paginiChinese Vocabulary AnimalsWei LeeÎncă nu există evaluări
- Diversity IN Living WorldDocument36 paginiDiversity IN Living WorldAnuradha PorwalÎncă nu există evaluări
- UntitledDocument41 paginiUntitledReham Ricka ValmonteÎncă nu există evaluări
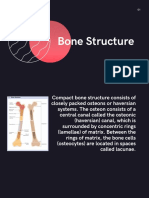
- Topic PPT Bone StructureDocument14 paginiTopic PPT Bone StructureMoonÎncă nu există evaluări
- Cat and Mouse 2Document2 paginiCat and Mouse 2Da MiánÎncă nu există evaluări