S-ar putea să vă placă și
- Family Nursing Care PlanDocument1 paginăFamily Nursing Care Planmerryechevarria100% (9)
- Literature Review On Patient Satisfaction With Nursing CareDocument6 paginiLiterature Review On Patient Satisfaction With Nursing Carec5jbmre7Încă nu există evaluări
- Doctors Nurses Overcome Workplace HierarchiesDocument6 paginiDoctors Nurses Overcome Workplace HierarchiesAndres CarreraÎncă nu există evaluări
- Nur417 Benchmarking ProjectDocument12 paginiNur417 Benchmarking Projectapi-529373199Încă nu există evaluări
- Ebook Nursing CollectionDocument88 paginiEbook Nursing CollectionTiffany MartinezÎncă nu există evaluări
- Transcultural NursingDocument22 paginiTranscultural NursingTricia Anne Paloma VergaraÎncă nu există evaluări
- NCM 107 CompleteDocument35 paginiNCM 107 CompleteKamx Mohammed100% (2)
- Research Paper On Service Quality in HospitalsDocument5 paginiResearch Paper On Service Quality in Hospitalsskpcijbkf100% (1)
- Evidence Based Practice Research Paper TopicsDocument7 paginiEvidence Based Practice Research Paper Topicsefh4m77n100% (1)
- Mathematical Modelling in Health Care: Karnon, J., Mark Mackay and T.M. MillsDocument13 paginiMathematical Modelling in Health Care: Karnon, J., Mark Mackay and T.M. MillsTyas AgustinaÎncă nu există evaluări
- The Positive Impact of Continuous ImprovementDocument15 paginiThe Positive Impact of Continuous ImprovementMane DaralÎncă nu există evaluări
- Thesis Statement On HospitalsDocument5 paginiThesis Statement On Hospitalsbkrj0a1k100% (1)
- Review of Related Literature Patient SatisfactionDocument8 paginiReview of Related Literature Patient Satisfactionequnruwgf100% (1)
- Literature Review of Patient Satisfaction SurveysDocument8 paginiLiterature Review of Patient Satisfaction Surveysamjatzukg100% (1)
- Health Care's Service FanaticsDocument17 paginiHealth Care's Service Fanaticsali1860Încă nu există evaluări
- Thesis LSHTMDocument6 paginiThesis LSHTMdqaucoikd100% (2)
- Clinical Decision Support Systems (CDSSS) Name Year AffiliationDocument16 paginiClinical Decision Support Systems (CDSSS) Name Year AffiliationPATRICK OTIATOÎncă nu există evaluări
- Review of Literature Patient SatisfactionDocument5 paginiReview of Literature Patient Satisfactioneldcahvkg100% (1)
- 2010 Seven Ways To No Delays FINAL (Low-Res)Document24 pagini2010 Seven Ways To No Delays FINAL (Low-Res)Ruby SharmaÎncă nu există evaluări
- Nurse Practitioner Research PaperDocument8 paginiNurse Practitioner Research Paperqzafzzhkf100% (1)
- The Top 6 Examples of Quality Improvement in HealthcareDocument7 paginiThe Top 6 Examples of Quality Improvement in HealthcareDennis Junior ChorumaÎncă nu există evaluări
- Health Care's Service Fanatics (HBR)Document19 paginiHealth Care's Service Fanatics (HBR)Edgard SantosÎncă nu există evaluări
- Family-Centred Care in Paediatric and Neonatal Nursing - A Literature ReviewDocument4 paginiFamily-Centred Care in Paediatric and Neonatal Nursing - A Literature Reviewhyzypif0gif3Încă nu există evaluări
- Rapid Response Team Whitepaper With Intro UPDATEDDocument24 paginiRapid Response Team Whitepaper With Intro UPDATEDHari Mas KuncoroÎncă nu există evaluări
- Liedel Survey of Time Project11-4Document9 paginiLiedel Survey of Time Project11-4Sherif ElkadyÎncă nu există evaluări
- Literature Review Developing Competencies For Health Promotion Deliverable 3bDocument10 paginiLiterature Review Developing Competencies For Health Promotion Deliverable 3bxfeivdsifÎncă nu există evaluări
- Original 1Document5 paginiOriginal 1Dhiyon CoconÎncă nu există evaluări
- Patient Satisfaction SurveyDocument113 paginiPatient Satisfaction SurveyCherry Mae L. Villanueva100% (1)
- Tourist Satisfaction DissertationDocument7 paginiTourist Satisfaction DissertationHelpInWritingPaperUK100% (1)
- Journal Article Critique Nursing 665Document5 paginiJournal Article Critique Nursing 665api-214213767Încă nu există evaluări
- Patient Satisfaction Survey Literature ReviewDocument7 paginiPatient Satisfaction Survey Literature Reviewea8142xb100% (1)
- Literature Review Person Centred CareDocument5 paginiLiterature Review Person Centred Careafdtszfwb100% (1)
- Ctu Medication ManagementnovoiceDocument12 paginiCtu Medication Managementnovoiceapi-240028260Încă nu există evaluări
- Project ReportDocument41 paginiProject ReportAnoop PunathilÎncă nu există evaluări
- Qsen PresentationDocument26 paginiQsen Presentationapi-235633705100% (1)
- HW5Document4 paginiHW5Karthik GanesuniÎncă nu există evaluări
- Sample Nursing Student Research PaperDocument8 paginiSample Nursing Student Research Paperfvf8gc78100% (1)
- DRG AssignmentDocument12 paginiDRG Assignmentavpnqvfng100% (1)
- Translating Clinical Guidelines Into Practice Challenges and Opportunities in A Dynamic Health Care EnvironmentDocument5 paginiTranslating Clinical Guidelines Into Practice Challenges and Opportunities in A Dynamic Health Care EnvironmentMorris KiioÎncă nu există evaluări
- Customer Perception Towards Private HospitalsDocument29 paginiCustomer Perception Towards Private HospitalsBilal Ah Parray90% (10)
- Nursing Assistant Research PaperDocument6 paginiNursing Assistant Research Paperafeeotove100% (1)
- 556-Appropriateness of Clinical Decision Support - Final White Paper-Wei WuDocument15 pagini556-Appropriateness of Clinical Decision Support - Final White Paper-Wei Wuapi-398506399Încă nu există evaluări
- Group 4 - Shouldice HospitalDocument9 paginiGroup 4 - Shouldice HospitalRithwik PrathapÎncă nu există evaluări
- RN Journal Literature Review Safe Nurse StaffingDocument4 paginiRN Journal Literature Review Safe Nurse Staffinggw07z0j5100% (1)
- RetrieveDocument7 paginiRetrieveGestión Clínica SeguraÎncă nu există evaluări
- Full Download Test Bank For Evidence Based Practice For Nursing and Healthcare Quality Improvement 1st Edition by Lobiondo Wood PDF Full ChapterDocument36 paginiFull Download Test Bank For Evidence Based Practice For Nursing and Healthcare Quality Improvement 1st Edition by Lobiondo Wood PDF Full Chapterpapismlepal.b8x1100% (16)
- Evidenced Based Nursing PracticeDocument7 paginiEvidenced Based Nursing PracticeKim ViñasÎncă nu există evaluări
- Improving Length of Stay:: What Can Hospitals Do?Document28 paginiImproving Length of Stay:: What Can Hospitals Do?Ahmed M. HassenÎncă nu există evaluări
- EDPerformanceMeasures ConsensusStatementDocument10 paginiEDPerformanceMeasures ConsensusStatementMarwa El SayedÎncă nu există evaluări
- Quality and Safety Synthesis PaperDocument6 paginiQuality and Safety Synthesis Paperapi-252807964Încă nu există evaluări
- Discussion For Module 7Document3 paginiDiscussion For Module 7Hussain MirzaÎncă nu există evaluări
- Managing Healthcare QualityDocument7 paginiManaging Healthcare QualityTooba SiddiquiÎncă nu există evaluări
- Improving Efficiency and Value in Health Care IntroductionDocument6 paginiImproving Efficiency and Value in Health Care IntroductionCoondog JonesÎncă nu există evaluări
- Healthcare Service Lines - The State of The Future by Dr. Jon BurroughsDocument10 paginiHealthcare Service Lines - The State of The Future by Dr. Jon BurroughsAbidi HichemÎncă nu există evaluări
- Root Cause Analysis of A Safety ProblemDocument6 paginiRoot Cause Analysis of A Safety Problemapi-300602911Încă nu există evaluări
- In Patient Satisfaction Survey-How Does It Help Our Health Care Delivery System (The Patient, The Health Care Giver and The Organization) ?Document10 paginiIn Patient Satisfaction Survey-How Does It Help Our Health Care Delivery System (The Patient, The Health Care Giver and The Organization) ?Pallavi PalluÎncă nu există evaluări
- Evidence-Based Nursing: The 5 Steps of EBNDocument13 paginiEvidence-Based Nursing: The 5 Steps of EBNRanjith RgtÎncă nu există evaluări
- Studer Group Toolkit - HcahpsDocument22 paginiStuder Group Toolkit - Hcahpscervelo_6927100% (2)
- Research Paper On Registered NursesDocument6 paginiResearch Paper On Registered Nursesc9hpjcb3100% (1)
- Nursing Sciences English Department, Second YearDocument11 paginiNursing Sciences English Department, Second Yearmosto mostoÎncă nu există evaluări
- Dissertation Clinical TrialsDocument5 paginiDissertation Clinical TrialsCanSomeoneWriteMyPaperForMeSingapore100% (1)
- Literature Review Patient Centered CareDocument7 paginiLiterature Review Patient Centered Careeowcnerke100% (1)
- Hospital Transformation: From Failure to Success and BeyondDe la EverandHospital Transformation: From Failure to Success and BeyondÎncă nu există evaluări
- Efficient Radiology: How to Optimize Radiology OperationsDe la EverandEfficient Radiology: How to Optimize Radiology OperationsÎncă nu există evaluări
- Desperdicios Procesos ServiciosDocument3 paginiDesperdicios Procesos ServiciosAndrés AvilésÎncă nu există evaluări
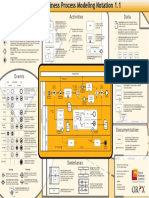
- BPMN Poster PDFDocument1 paginăBPMN Poster PDFAndrés AvilésÎncă nu există evaluări
- Linear Programming IntroductionDocument22 paginiLinear Programming IntroductionAndrés AvilésÎncă nu există evaluări
- What Is Management?Document5 paginiWhat Is Management?Andrés AvilésÎncă nu există evaluări
- Chapter 01 Marketing Managing Profitable Customer RelationshipsDocument21 paginiChapter 01 Marketing Managing Profitable Customer RelationshipsAndrés Avilés100% (1)
- Definition of AccountingDocument2 paginiDefinition of AccountingAndrés AvilésÎncă nu există evaluări
- How Do You Create A Current State Value Stream Map?Document17 paginiHow Do You Create A Current State Value Stream Map?Andrés AvilésÎncă nu există evaluări
- Chap 1-S1 PDFDocument15 paginiChap 1-S1 PDFAndrés AvilésÎncă nu există evaluări
- What Is Kanban?Document17 paginiWhat Is Kanban?Andrés AvilésÎncă nu există evaluări
- Far Eastern University-Dr. Nicanor Reyes Medical FoundationDocument3 paginiFar Eastern University-Dr. Nicanor Reyes Medical FoundationJoseph Raymund Fabian HuelarÎncă nu există evaluări
- Cm3 - Cu20 Guidelines of An Effective Interview and Health HistoryDocument8 paginiCm3 - Cu20 Guidelines of An Effective Interview and Health HistoryHannah Mae BabidaÎncă nu există evaluări
- G2 3rd Revision FIRST HALFDocument20 paginiG2 3rd Revision FIRST HALFSbs Nhanxzkie Jountey MushroomxzÎncă nu există evaluări
- Delegation NCLEX-RNDocument3 paginiDelegation NCLEX-RNPrince K. Tailey100% (1)
- NP ResumeDocument3 paginiNP Resumeapi-554096544Încă nu există evaluări
- Nurs 440 Change ModelDocument2 paginiNurs 440 Change Modelapi-249918909Încă nu există evaluări
- Brooks 2017Document37 paginiBrooks 2017Fredynata CasanaÎncă nu există evaluări
- Nursing ProcessDocument10 paginiNursing ProcessBrandy SangurahÎncă nu există evaluări
- Job Application Letter Nurses ExamplesDocument7 paginiJob Application Letter Nurses Examplesguj0zukyven2100% (2)
- Autumn Gettings ResumeDocument2 paginiAutumn Gettings Resumeapi-663930784Încă nu există evaluări
- 2009 Commencement ExercisesDocument30 pagini2009 Commencement Exerciseslhoydskiee100% (1)
- Soft Skills Essay - SmithDocument3 paginiSoft Skills Essay - Smithapi-495996370Încă nu există evaluări
- NCPDocument6 paginiNCPRyan John Bito-onÎncă nu există evaluări
- Career DevelopmentDocument11 paginiCareer DevelopmentLee BuelaÎncă nu există evaluări
- 2nd Reporters 119Document9 pagini2nd Reporters 119Ellen Joyce FlorÎncă nu există evaluări
- N117 SyllabusDocument182 paginiN117 SyllabusNurdiansyahÎncă nu există evaluări
- Answer KeyDocument25 paginiAnswer KeySha MetlangÎncă nu există evaluări
- 20th Century NurseDocument5 pagini20th Century NurseMisch Yeen100% (1)
- Apa Paper 2nd SemesterDocument5 paginiApa Paper 2nd Semesterapi-268209871Încă nu există evaluări
- Chapter 27 Managing Your CareerDocument7 paginiChapter 27 Managing Your CareerLorene ReynoldsÎncă nu există evaluări
- Ps111 Spirituality 2010 eDocument4 paginiPs111 Spirituality 2010 enersitiulfahÎncă nu există evaluări
- Triage in Emergency Department Using ESi (5 Levels) Self Study 8.2015 in PDF Format For Email and PostingDocument52 paginiTriage in Emergency Department Using ESi (5 Levels) Self Study 8.2015 in PDF Format For Email and Postingdian prawita100% (1)
- Profile PDFDocument2 paginiProfile PDFsavan anvekarÎncă nu există evaluări
- Huddles: Patient Safety Essentials ToolkitDocument4 paginiHuddles: Patient Safety Essentials Toolkitamal aldhafeeriÎncă nu există evaluări
- Integrative Literature ReviewDocument17 paginiIntegrative Literature Reviewapi-426049026Încă nu există evaluări
- Nurse Practitioner Resume 2019Document7 paginiNurse Practitioner Resume 2019api-482787212Încă nu există evaluări