S-ar putea să vă placă și
- Drug StudyDocument5 paginiDrug StudyRai D. MacapantonÎncă nu există evaluări
- NCLEX: Pharmacology for Nurses: 100 Practice Questions with Rationales to help you Pass the NCLEX!De la EverandNCLEX: Pharmacology for Nurses: 100 Practice Questions with Rationales to help you Pass the NCLEX!Evaluare: 5 din 5 stele5/5 (4)
- Unit 1. Clinical PharmacyDocument5 paginiUnit 1. Clinical PharmacyAashish BhattaraiÎncă nu există evaluări
- Nursing Pharmacology Handouts For ZamboDocument7 paginiNursing Pharmacology Handouts For ZamboAlexa Abidin Oldenborg100% (8)
- CHN Drug StudyDocument10 paginiCHN Drug StudyJoshua Cyryll ComiaÎncă nu există evaluări
- Drug Study For Mefenamic Acid, Tramadol and CefuroximeDocument7 paginiDrug Study For Mefenamic Acid, Tramadol and CefuroximeChristian Karl B. LlanesÎncă nu există evaluări
- First Aid Does Not Just Promote Faster Recovery It Helps Save LivesDocument4 paginiFirst Aid Does Not Just Promote Faster Recovery It Helps Save LivesJoy Rosario100% (2)
- Pediatric Drug FormulationsDocument14 paginiPediatric Drug FormulationsJürgen FleischerÎncă nu există evaluări
- Lithium CarbonateDocument2 paginiLithium CarbonateArnzz AgbulosÎncă nu există evaluări
- Antidepressants and Antipsychotics NCLEX ReviewerDocument4 paginiAntidepressants and Antipsychotics NCLEX ReviewerRonÎncă nu există evaluări
- Jisha New CV Final 2Document5 paginiJisha New CV Final 2Mary JisÎncă nu există evaluări
- Methylprednisolone (Solu-Medrol) : Emergency MedicationsDocument3 paginiMethylprednisolone (Solu-Medrol) : Emergency MedicationsKdamnzÎncă nu există evaluări
- Bilastine (United States - Not Available) - Drug Information - UpToDateDocument13 paginiBilastine (United States - Not Available) - Drug Information - UpToDatekadioglu20Încă nu există evaluări
- Course Task 2Document2 paginiCourse Task 2John Elton TangpuzÎncă nu există evaluări
- TylenolDocument2 paginiTylenolAle_deCastroÎncă nu există evaluări
- Beta Karoten: (BAY Ta KARE Oh Teen)Document9 paginiBeta Karoten: (BAY Ta KARE Oh Teen)Nisa'ul KhoiriyahÎncă nu există evaluări
- Anticholinergic: Classification Generic Name Brand NameDocument6 paginiAnticholinergic: Classification Generic Name Brand NameKarina MadriagaÎncă nu există evaluări
- Drug StudyDocument9 paginiDrug StudyShane Arroyo100% (1)
- WEEK2 Course Task (ALFEREZ, DINIELA)Document4 paginiWEEK2 Course Task (ALFEREZ, DINIELA)DINIELA ALLAINE ALFEREZÎncă nu există evaluări
- Side Effects:: AtropineDocument7 paginiSide Effects:: AtropinekletadaÎncă nu există evaluări
- Pentazine, Phenazine, Phencen,, Phenoject-50, Prometh, Prorex, Prothazine, V-GanDocument34 paginiPentazine, Phenazine, Phencen,, Phenoject-50, Prometh, Prorex, Prothazine, V-GankotonashiÎncă nu există evaluări
- Drug Study Case Study PebsDocument6 paginiDrug Study Case Study PebsMichael John Gambong SalaÎncă nu există evaluări
- Drug 25Document17 paginiDrug 25carol_gigliotti24100% (1)
- Annexure - II Product DevelopmentDocument50 paginiAnnexure - II Product DevelopmentLife PearlÎncă nu există evaluări
- TrihexyphenidylDocument5 paginiTrihexyphenidylZepHemaÎncă nu există evaluări
- Legaspi Course Task 2Document7 paginiLegaspi Course Task 2FATIMA AIRA LEGASPIÎncă nu există evaluări
- Pharmacology PPDocument16 paginiPharmacology PPbridgetkabwe78Încă nu există evaluări
- Cardio DrugsDocument58 paginiCardio DrugsMARIA ROWENA VIA J. LUCENAÎncă nu există evaluări
- Meropenem - Drug Information - UpToDate-3Document8 paginiMeropenem - Drug Information - UpToDate-3Vh TRÎncă nu există evaluări
- AcetazolamideDocument1 paginăAcetazolamideKyuSheenÎncă nu există evaluări
- Anticholinergic: Anticholinergics: Generic and Brand NamesDocument6 paginiAnticholinergic: Anticholinergics: Generic and Brand NamesSaffery Gly LayuganÎncă nu există evaluări
- Generic Name: Albuterol Brand Name: Salbutamol, Proventil, Ventolin, Accuneb, Airet, Novo-SalbutamolDocument26 paginiGeneric Name: Albuterol Brand Name: Salbutamol, Proventil, Ventolin, Accuneb, Airet, Novo-SalbutamolAnna Joy Antone100% (1)
- Drugs Acting On The Endocrine System Hypothalmic and Pituitary AgentsDocument19 paginiDrugs Acting On The Endocrine System Hypothalmic and Pituitary AgentsAyna Salic PangarunganÎncă nu există evaluări
- 11 15Document8 pagini11 15Dinarkram Rabreca EculÎncă nu există evaluări
- Metoprolol Drug Prsentation: By, Rachel - J BSC Nursing 2 Year College of Nursing, Christian Fellowship HospitalDocument33 paginiMetoprolol Drug Prsentation: By, Rachel - J BSC Nursing 2 Year College of Nursing, Christian Fellowship HospitalRachel JohnÎncă nu există evaluări
- Pycnogenol Consumer/Patient Information SheetDocument1 paginăPycnogenol Consumer/Patient Information SheetDeboraNainggolanÎncă nu există evaluări
- Dipyrone (Metamizole) : Pronunciation Brand Names: InternationalDocument9 paginiDipyrone (Metamizole) : Pronunciation Brand Names: InternationalRismaya AminiÎncă nu există evaluări
- 5th Draft DrugsDocument7 pagini5th Draft DrugsShayne Jessemae AlmarioÎncă nu există evaluări
- 06 2014 Anticholinergic Agents - AtropineDocument6 pagini06 2014 Anticholinergic Agents - AtropinemodayearÎncă nu există evaluări
- HyrdrocortisoneDocument7 paginiHyrdrocortisoneRoseben SomidoÎncă nu există evaluări
- Pharmacology: By: Jan Michael Khalid L. Macarambon, RNDocument164 paginiPharmacology: By: Jan Michael Khalid L. Macarambon, RNJan MacarambonÎncă nu există evaluări
- Pharma 2014Document34 paginiPharma 2014backupuoload85Încă nu există evaluări
- AcetazolamideDocument25 paginiAcetazolamideDiwan AyuÎncă nu există evaluări
- Colobreathe-Spc enDocument30 paginiColobreathe-Spc enlamprinilÎncă nu există evaluări
- Cefadroxil (Cephalosporin Generasi I)Document5 paginiCefadroxil (Cephalosporin Generasi I)Yustia SariÎncă nu există evaluări
- Drugstudy and SoapieDocument17 paginiDrugstudy and SoapieYasi EcheniqueÎncă nu există evaluări
- Case Study No.4 The Telltale Heart: Group 2 Nuñez, Refuerzo, Abalos, Almonte, AlmueteDocument11 paginiCase Study No.4 The Telltale Heart: Group 2 Nuñez, Refuerzo, Abalos, Almonte, AlmueteRejeanne MonroyÎncă nu există evaluări
- Cu Task 2 PharmaDocument5 paginiCu Task 2 PharmaNiña ReyesÎncă nu există evaluări
- Respiratory Drugs Midterm ExamDocument10 paginiRespiratory Drugs Midterm ExamKevin VillaranteÎncă nu există evaluări
- UTD FosfomycinDocument5 paginiUTD FosfomycinfededelveliÎncă nu există evaluări
- PropoxypheneDocument3 paginiPropoxypheneapi-3797941Încă nu există evaluări
- Therapeutic: Urinary Tract Stimulants Pharmacologic: CholinergicDocument37 paginiTherapeutic: Urinary Tract Stimulants Pharmacologic: CholinergicApple MaeÎncă nu există evaluări
- Summary of Product CharacteristicDocument5 paginiSummary of Product Characteristicresearch universalÎncă nu există evaluări
- AmoxicillinDocument2 paginiAmoxicillindheng05Încă nu există evaluări
- Gastrointestinal DrugDocument29 paginiGastrointestinal DrugJeneyse Ajap BalcenaÎncă nu există evaluări
- Anti TB DrugsDocument22 paginiAnti TB DrugsIsmael JaaniÎncă nu există evaluări
- Discussion Topics 1Document6 paginiDiscussion Topics 1Jojo JustoÎncă nu există evaluări
- Drug StudyDocument186 paginiDrug StudyTheresa Sombilla FacunlaÎncă nu există evaluări
- DRUG and IVF StudyDocument4 paginiDRUG and IVF StudyJohanna Camelle Insong MonteronÎncă nu există evaluări
- Cefmetazole (Cephalosporin Generasi II)Document4 paginiCefmetazole (Cephalosporin Generasi II)Afdelina RizkyÎncă nu există evaluări
- Identify The Cause To Control The SymptomDocument3 paginiIdentify The Cause To Control The SymptomKimberly Joy GregorioÎncă nu există evaluări
- Unit 1Document15 paginiUnit 1kunalÎncă nu există evaluări
- The Best Practice Is The Lowest Effective Dose Your Third Psychiatric Consultation: Diet, Exercise, and Sleep Trump Medications Medication is the Last Option Your Fourth Psychiatric ConsultationDe la EverandThe Best Practice Is The Lowest Effective Dose Your Third Psychiatric Consultation: Diet, Exercise, and Sleep Trump Medications Medication is the Last Option Your Fourth Psychiatric ConsultationÎncă nu există evaluări
- Retdem 6 MarchDocument2 paginiRetdem 6 MarchCurtney PedriaÎncă nu există evaluări
- MetabolicsyndDocument37 paginiMetabolicsyndShanooha MansoorÎncă nu există evaluări
- Prodrug Delivery PDFDocument6 paginiProdrug Delivery PDFanantachoudhuryÎncă nu există evaluări
- Pharmacy Board ExamDocument2 paginiPharmacy Board ExamRhealyn LegaspiÎncă nu există evaluări
- Medical Cannabisin Israelseptember 20111Document7 paginiMedical Cannabisin Israelseptember 20111cannajoyÎncă nu există evaluări
- Padlan Getigan and PartnersDocument4 paginiPadlan Getigan and PartnersMichaelandKaye DanaoÎncă nu există evaluări
- Week 12 Short Answer QuestionsDocument2 paginiWeek 12 Short Answer Questionschristinaj98Încă nu există evaluări
- Opioid Abusers Prefer Hydrocodone or Oxycodone For Different ReasonsDocument1 paginăOpioid Abusers Prefer Hydrocodone or Oxycodone For Different Reasonsobx4everÎncă nu există evaluări
- ResearchDocument34 paginiResearchBenjamin TantiansuÎncă nu există evaluări
- Pulmonary Function TestingDocument25 paginiPulmonary Function TestingZohaib SiddiquiÎncă nu există evaluări
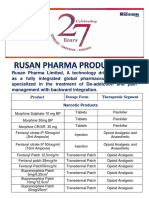
- Rusan Pharma Product ListDocument4 paginiRusan Pharma Product ListSanjay SharmaÎncă nu există evaluări
- Drug Card GardasilDocument2 paginiDrug Card GardasilJuliaÎncă nu există evaluări
- (Antianginal Drugs) : Faculty of Pharmacy - Menoufia University Code (PC805)Document3 pagini(Antianginal Drugs) : Faculty of Pharmacy - Menoufia University Code (PC805)sfsffÎncă nu există evaluări
- Klinger 2014Document4 paginiKlinger 2014Alejandra CachoÎncă nu există evaluări
- Alevo Alkem (Ulticare) (Levofloxacin) : Strength Presentation PriceDocument21 paginiAlevo Alkem (Ulticare) (Levofloxacin) : Strength Presentation Pricepathan mohidÎncă nu există evaluări
- CDER Fast Track Products Approved Since 1998 Through June 1, 2010Document5 paginiCDER Fast Track Products Approved Since 1998 Through June 1, 2010dianÎncă nu există evaluări
- Question Bank BiopharmDocument6 paginiQuestion Bank BiopharmHrushikesh JadhavÎncă nu există evaluări
- How To Prescribe Drug For DentistsDocument22 paginiHow To Prescribe Drug For DentistsahmedÎncă nu există evaluări
- Bioavailability and Pharmacokinetics of Oral MeloxDocument12 paginiBioavailability and Pharmacokinetics of Oral MeloxCandy HLÎncă nu există evaluări
- Drug Dose CalculationsDocument13 paginiDrug Dose CalculationsPrince AliÎncă nu există evaluări
- PT - Permata Delta Agung: Halaman: (All)Document35 paginiPT - Permata Delta Agung: Halaman: (All)abdul husainÎncă nu există evaluări
- CefazolinDocument3 paginiCefazolinintrovert ikonÎncă nu există evaluări
- Set Rec Pic 829Document2 paginiSet Rec Pic 829Peter SalimÎncă nu există evaluări
- Jawaharlal Nehru Technological University Hyderabad: Date& Day R17 R16 R15 R13 R09Document1 paginăJawaharlal Nehru Technological University Hyderabad: Date& Day R17 R16 R15 R13 R09TempÎncă nu există evaluări
- Clinical Pharmacology of Antibiotics - PMCDocument19 paginiClinical Pharmacology of Antibiotics - PMCJosette LeyvaÎncă nu există evaluări
- NCP, DTR, HTP and Play TherapyDocument4 paginiNCP, DTR, HTP and Play TherapyQuiannë Delos ReyesÎncă nu există evaluări