S-ar putea să vă placă și
- Neoplasms of TestisDocument26 paginiNeoplasms of TestisFeddyFebriyantoManurungÎncă nu există evaluări
- Epidemiology of Ovarian Cancer: A ReviewDocument24 paginiEpidemiology of Ovarian Cancer: A ReviewWiedya kristiantiÎncă nu există evaluări
- Pathology of Germ Cell Tumors of The TestisDocument14 paginiPathology of Germ Cell Tumors of The TestisAnonymous be1sWu6l6Încă nu există evaluări
- Pathogenesis of Testicular Germ Cell Tumours: Leendert H. J. Looijenga and J. Wolter OosterhuisDocument11 paginiPathogenesis of Testicular Germ Cell Tumours: Leendert H. J. Looijenga and J. Wolter OosterhuisLatansa DinaÎncă nu există evaluări
- 6 Tumors IntroductionDocument101 pagini6 Tumors IntroductionReZky MusliminÎncă nu există evaluări
- Clear Cell CADocument2 paginiClear Cell CAOscar HalumÎncă nu există evaluări
- Oncology Toribio Augene SecFDocument9 paginiOncology Toribio Augene SecFAugene ToribioÎncă nu există evaluări
- Testicular CancerDocument11 paginiTesticular CancercilengsaiÎncă nu există evaluări
- Neoplasia ExamDocument9 paginiNeoplasia ExamYheng Gaosaii100% (1)
- Semi No MaDocument2 paginiSemi No MaDea Prista AgathaÎncă nu există evaluări
- MR 28 Agustus-1Document7 paginiMR 28 Agustus-1BramaÎncă nu există evaluări
- Finger Clubbing and A Lung MassDocument5 paginiFinger Clubbing and A Lung MassSeptinaAyuSamsiatiÎncă nu există evaluări
- TESTICULAR CANCER BookletDocument33 paginiTESTICULAR CANCER BookletCheeBrendaÎncă nu există evaluări
- POGS Practice Bulletin 3 FINALDocument6 paginiPOGS Practice Bulletin 3 FINALAileen TombocÎncă nu există evaluări
- G Path-NeoplasiaDocument60 paginiG Path-Neoplasiachouchou124Încă nu există evaluări
- RPB14150079015Document5 paginiRPB14150079015Ijupbs IjupbsÎncă nu există evaluări
- Jurnal Kanker TestisDocument9 paginiJurnal Kanker TestisDiatni FibriÎncă nu există evaluări
- Testis CancerDocument9 paginiTestis CancerMuhammad Tawfiq ZamriÎncă nu există evaluări
- 624 PDFDocument9 pagini624 PDFTri AryantiÎncă nu există evaluări
- Subject Date Professor Sbobinatore: (Armando Muro) ReviewerDocument10 paginiSubject Date Professor Sbobinatore: (Armando Muro) ReviewerÁngel Parra CominoÎncă nu există evaluări
- Kurman 2013Document6 paginiKurman 2013adevanshi3399Încă nu există evaluări
- Medsci 06 00031 PDFDocument113 paginiMedsci 06 00031 PDFCarolina VillalobosÎncă nu există evaluări
- Asal CA OvarianDocument3 paginiAsal CA OvarianBenyamin Rakhmatsyah TitaleyÎncă nu există evaluări
- Smith 2017Document14 paginiSmith 2017Evelynππ θσυÎncă nu există evaluări
- Testicular CancerDocument12 paginiTesticular Cancerghost_724Încă nu există evaluări
- Lesions Infertile: Precancerous of The Cervix Uteri in WomenDocument2 paginiLesions Infertile: Precancerous of The Cervix Uteri in WomenGede S PutrawanÎncă nu există evaluări
- The Unitarian or Trophoblastic Thesis of CancerDocument32 paginiThe Unitarian or Trophoblastic Thesis of Canceruge9Încă nu există evaluări
- Biochemistry of CrytorchidismDocument21 paginiBiochemistry of CrytorchidismGabrielÎncă nu există evaluări
- ReviewDocument5 paginiReviewerickmattosÎncă nu există evaluări
- Papillary Thyroid CarcinomaDocument9 paginiPapillary Thyroid CarcinomaELinkTulusÎncă nu există evaluări
- Praktikum Reproduksi 2Document46 paginiPraktikum Reproduksi 2Andika Tatag100% (1)
- Navigation Search Cancer (Disambiguation) : (Intrusion On and Destruction of Adjacent Tissues), and SometimesDocument23 paginiNavigation Search Cancer (Disambiguation) : (Intrusion On and Destruction of Adjacent Tissues), and Sometimesmariannec_3Încă nu există evaluări
- CancerDocument14 paginiCancerNano AlmukasabyÎncă nu există evaluări
- Dunn RefDocument47 paginiDunn RefFlorencia Chandrika HalimÎncă nu există evaluări
- Giant Uterine Leiomyoma - Case Report and Review of LiteratureDocument3 paginiGiant Uterine Leiomyoma - Case Report and Review of LiteratureMan ManuelÎncă nu există evaluări
- Testis and EpididymisDocument15 paginiTestis and EpididymisJake MillerÎncă nu există evaluări
- Tumori Testisa PDFDocument14 paginiTumori Testisa PDFVuk MilutinovićÎncă nu există evaluări
- Neoplasma TestisDocument3 paginiNeoplasma TestisFalira MuthiaÎncă nu există evaluări
- CarcinogenicityDocument66 paginiCarcinogenicityNormana ZureikatÎncă nu există evaluări
- Testicular Cancer (Teratoma Testis)Document7 paginiTesticular Cancer (Teratoma Testis)Witha Lestari AdethiaÎncă nu există evaluări
- Presença de Beta III Nas Células de Kulchitsky Sugere Sua Origem Subventricular Do SNCDocument3 paginiPresença de Beta III Nas Células de Kulchitsky Sugere Sua Origem Subventricular Do SNCFedericoDiGiovanniÎncă nu există evaluări
- Adenocarcinoma Borderline OvarioDocument18 paginiAdenocarcinoma Borderline OvarioIsaac MaderoÎncă nu există evaluări
- Metastases To The Thyroid: A Review of The Literature From The Last Decade Chung2012-2Document11 paginiMetastases To The Thyroid: A Review of The Literature From The Last Decade Chung2012-2Pavel GonzálezÎncă nu există evaluări
- Sacrococcygeal Teratoma A Tumor at The Center of EmbryogenesisDocument8 paginiSacrococcygeal Teratoma A Tumor at The Center of EmbryogenesisLuis Ruelas SanchezÎncă nu există evaluări
- Original Research ReportDocument4 paginiOriginal Research ReportSehrish SiddiqueÎncă nu există evaluări
- Neonatal Extra-Renal Wilm's Tumour: Division of Paediatric Surgery, Aga Khan University Hospital, KarachiDocument2 paginiNeonatal Extra-Renal Wilm's Tumour: Division of Paediatric Surgery, Aga Khan University Hospital, Karachidydy_7193Încă nu există evaluări
- Cancers Make Their Own Luck - Theories of Cancer OriginsDocument15 paginiCancers Make Their Own Luck - Theories of Cancer Originszhe zhÎncă nu există evaluări
- Papillary Thyroid CarcinomaDocument17 paginiPapillary Thyroid CarcinomaEster Sibarani100% (2)
- Theories of Endometrial CarcinogenesisDocument14 paginiTheories of Endometrial CarcinogenesisRisti SFÎncă nu există evaluări
- Colon Cancer: Risk Factors and Therapeutic ApproachesDocument11 paginiColon Cancer: Risk Factors and Therapeutic ApproachesCentral Asian StudiesÎncă nu există evaluări
- Near-Infrared Raman Spectroscopy For TheDocument12 paginiNear-Infrared Raman Spectroscopy For TheAlberto Carlos Espinosa GaravitoÎncă nu există evaluări
- NATIONAL CANCER CONTROL PROGRAMM 2 (Prakash)Document19 paginiNATIONAL CANCER CONTROL PROGRAMM 2 (Prakash)angayarkanni100% (1)
- Incidence A N D Case-Control Study: Ovarian CancerDocument7 paginiIncidence A N D Case-Control Study: Ovarian CancerHannah SteinmetzÎncă nu există evaluări
- PG Art 34580-10Document15 paginiPG Art 34580-10Horia MineaÎncă nu există evaluări
- Micrornas and Recent Insights Into Pediatric Ovarian CancersDocument10 paginiMicrornas and Recent Insights Into Pediatric Ovarian CancersingeÎncă nu există evaluări
- Benign Cystic TeratomaDocument3 paginiBenign Cystic TeratomaLisa Dwipurnamasari TobingÎncă nu există evaluări
- Managing The Risk of Cancer in Cowden Syndrome: A Case ReportDocument4 paginiManaging The Risk of Cancer in Cowden Syndrome: A Case ReportKaisun TeoÎncă nu există evaluări
- Biology ProjectDocument6 paginiBiology ProjectBemnet TayeÎncă nu există evaluări
- Animal CellDocument7 paginiAnimal CellLezircYojDapmalÎncă nu există evaluări
- Lecture 1Document39 paginiLecture 1Mohammed SindiÎncă nu există evaluări
- Exercise Cell As The Basic Unit of Living ThingsDocument16 paginiExercise Cell As The Basic Unit of Living ThingsHidayatul ZawawiÎncă nu există evaluări
- Bolo - Dakabadonebuli - Book 2Document152 paginiBolo - Dakabadonebuli - Book 2sasa sasadzeÎncă nu există evaluări
- SHS STEM Bio1 Q1 Week 1 Module 2 Cell Structure and Functions 1Document17 paginiSHS STEM Bio1 Q1 Week 1 Module 2 Cell Structure and Functions 1Dette Dominic Ballano67% (3)
- Horizontal Gene Transfer in Eukaryotic Evolution - Nature Reviews Genetics - 2008Document14 paginiHorizontal Gene Transfer in Eukaryotic Evolution - Nature Reviews Genetics - 2008carlos murciaÎncă nu există evaluări
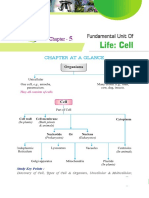
- Chapter at A Glance: Study Key PointsDocument14 paginiChapter at A Glance: Study Key PointssatishÎncă nu există evaluări
- Cells R UsDocument2 paginiCells R Usapi-264011999Încă nu există evaluări
- The Cell Structure and TaxonomyDocument10 paginiThe Cell Structure and TaxonomyKingJayson Pacman06Încă nu există evaluări
- Flashcards - Topic 17 Inheritance - CAIE Biology IGCSEDocument75 paginiFlashcards - Topic 17 Inheritance - CAIE Biology IGCSESabbath the sign of GodÎncă nu există evaluări
- DNA Programming Kit Manual PDFDocument65 paginiDNA Programming Kit Manual PDFavrajamohamedÎncă nu există evaluări
- Biomolecules and Cells NotesDocument81 paginiBiomolecules and Cells NotesLily RobinsonÎncă nu există evaluări
- Expert MdcatDocument4 paginiExpert Mdcathely shahÎncă nu există evaluări
- Science Biology 11-12 Q1Document9 paginiScience Biology 11-12 Q1Zhering RodulfoÎncă nu există evaluări
- Review of Medical Microbiology and Immunology 17th Edition (Medicalstudyzone - Com)Document1.016 paginiReview of Medical Microbiology and Immunology 17th Edition (Medicalstudyzone - Com)FaizÎncă nu există evaluări
- Cell Biology: InstructorDocument20 paginiCell Biology: Instructorahmed mediaÎncă nu există evaluări
- Samuelson - Textbook of Veterinary HistologyDocument710 paginiSamuelson - Textbook of Veterinary HistologyValentina Aguirre LópezÎncă nu există evaluări
- Lab 2 - InstructionsDocument16 paginiLab 2 - InstructionsCazzel AvilesÎncă nu există evaluări
- FET CP 1 Cell Structure & FunctionsDocument220 paginiFET CP 1 Cell Structure & FunctionsFarhat GirangÎncă nu există evaluări
- AS Level Biology Notes 2015 PDFDocument298 paginiAS Level Biology Notes 2015 PDFali hyd100% (1)
- G. Biology PPT Chapter 1-6new1Document238 paginiG. Biology PPT Chapter 1-6new1Alemayehu MelkamuuÎncă nu există evaluări
- Eukaryotic Chromosome Structure PDFDocument2 paginiEukaryotic Chromosome Structure PDFRachelÎncă nu există evaluări
- Choose The Correct AnswerDocument8 paginiChoose The Correct AnswerBLlahniesss Love KenÎncă nu există evaluări
- Neet Question Paper 2021 Code O1Document71 paginiNeet Question Paper 2021 Code O1Deev SoniÎncă nu există evaluări
- Gallery WalkDocument12 paginiGallery WalkPaul Hudson MackÎncă nu există evaluări
- 1.2 Ultrastructure of Cells: ProkaryotesDocument8 pagini1.2 Ultrastructure of Cells: Prokaryotesdavid tsaiÎncă nu există evaluări
- Actividad MitosisDocument6 paginiActividad MitosisVanesaÎncă nu există evaluări
- XXXXXXXXDocument17 paginiXXXXXXXXRicardo LazoÎncă nu există evaluări
- Topic 3 - Cellular Level of OrganizationDocument6 paginiTopic 3 - Cellular Level of OrganizationAdeyinka OluyoleÎncă nu există evaluări
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)De la EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Evaluare: 3 din 5 stele3/5 (1)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDe la EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDEvaluare: 5 din 5 stele5/5 (2)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDe la EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityEvaluare: 4 din 5 stele4/5 (29)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDe la EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionEvaluare: 4 din 5 stele4/5 (404)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDe la EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsÎncă nu există evaluări
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDe la EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedEvaluare: 5 din 5 stele5/5 (81)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDe la EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeEvaluare: 2 din 5 stele2/5 (1)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessDe la EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessEvaluare: 4.5 din 5 stele4.5/5 (328)
- The Obesity Code: Unlocking the Secrets of Weight LossDe la EverandThe Obesity Code: Unlocking the Secrets of Weight LossEvaluare: 4 din 5 stele4/5 (6)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDe la EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDe la EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisEvaluare: 4.5 din 5 stele4.5/5 (42)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDe la EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsEvaluare: 4 din 5 stele4/5 (4)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDe la EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsEvaluare: 5 din 5 stele5/5 (1)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeDe la EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeEvaluare: 4.5 din 5 stele4.5/5 (253)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.De la EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Evaluare: 4.5 din 5 stele4.5/5 (110)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDe la EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityEvaluare: 4 din 5 stele4/5 (5)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisDe la EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisEvaluare: 4 din 5 stele4/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryDe la EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryEvaluare: 4 din 5 stele4/5 (45)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDe la EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsEvaluare: 4.5 din 5 stele4.5/5 (170)
- Summary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedDe la EverandSummary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedEvaluare: 4 din 5 stele4/5 (61)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesDe la EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesEvaluare: 4.5 din 5 stele4.5/5 (1412)
- How to ADHD: The Ultimate Guide and Strategies for Productivity and Well-BeingDe la EverandHow to ADHD: The Ultimate Guide and Strategies for Productivity and Well-BeingEvaluare: 1 din 5 stele1/5 (1)
- The Marshmallow Test: Mastering Self-ControlDe la EverandThe Marshmallow Test: Mastering Self-ControlEvaluare: 4.5 din 5 stele4.5/5 (59)