S-ar putea să vă placă și
- Diet, Nutrition and The Prevention of OsteoporosisDocument17 paginiDiet, Nutrition and The Prevention of OsteoporosisGuruh FitriantoÎncă nu există evaluări
- Manajemen-Keperawatan - Vol-2-No-1.5-16-beban KerjaDocument12 paginiManajemen-Keperawatan - Vol-2-No-1.5-16-beban KerjaAnonymous 12ikjveo7Încă nu există evaluări
- 5256 10167 1 SMDocument9 pagini5256 10167 1 SMAnonymous 12ikjveo7Încă nu există evaluări
- Cirrhosis and Chronic Liver FailureDocument7 paginiCirrhosis and Chronic Liver FailureCamilla DanielleÎncă nu există evaluări
- Menu KankerDocument2 paginiMenu KankerAnonymous 12ikjveo7Încă nu există evaluări
- LED TMBHNDocument9 paginiLED TMBHNAnonymous 12ikjveo7Încă nu există evaluări
- Skin TestingDocument2 paginiSkin TestingBeningPutriRamadhaniUsmanÎncă nu există evaluări
- Nutritional Profile of Indian Vegetarian Diets - The Indian Migration Study (IMS)Document9 paginiNutritional Profile of Indian Vegetarian Diets - The Indian Migration Study (IMS)Anonymous 12ikjveo7Încă nu există evaluări
- The Impact of Religious Fasting On Human Health.Document9 paginiThe Impact of Religious Fasting On Human Health.Alberto Kenyo Riofrio PalaciosÎncă nu există evaluări
- Jawaban BSNDocument1 paginăJawaban BSNAnonymous 12ikjveo7Încă nu există evaluări
- The Impact of Religious Fasting On Human Health.Document9 paginiThe Impact of Religious Fasting On Human Health.Alberto Kenyo Riofrio PalaciosÎncă nu există evaluări
- 9305768Document10 pagini9305768Anonymous 12ikjveo7Încă nu există evaluări
- Nutritional Profile of Indian Vegetarian Diets - The Indian Migration Study (IMS)Document9 paginiNutritional Profile of Indian Vegetarian Diets - The Indian Migration Study (IMS)Anonymous 12ikjveo7Încă nu există evaluări
- 05 N022 47937Document24 pagini05 N022 47937Anonymous 12ikjveo7Încă nu există evaluări
- Eating Behaviors: Keith J. Zullig, Molly R. Matthews-Ewald, Robert F. ValoisDocument6 paginiEating Behaviors: Keith J. Zullig, Molly R. Matthews-Ewald, Robert F. ValoisAnonymous 12ikjveo7Încă nu există evaluări
- SSMJ Vol 6 1 TuberculosisDocument3 paginiSSMJ Vol 6 1 TuberculosisAnonymous 12ikjveo7Încă nu există evaluări
- Wajib - Tuberculosis - Pathophysiology, Clinical Features, and DiagnosisDocument12 paginiWajib - Tuberculosis - Pathophysiology, Clinical Features, and DiagnosisnurulahdiahÎncă nu există evaluări
- 1 s2.0 S0899900714004237 MainDocument9 pagini1 s2.0 S0899900714004237 MainAnonymous 12ikjveo7Încă nu există evaluări
- Eating Behaviors: Jung Su Lee, Gita Mishra, Kunihiko Hayashi, Etsuko Watanabe, Katsumi Mori, Kiyoshi KawakuboDocument5 paginiEating Behaviors: Jung Su Lee, Gita Mishra, Kunihiko Hayashi, Etsuko Watanabe, Katsumi Mori, Kiyoshi KawakuboAnonymous 12ikjveo7Încă nu există evaluări
- 1 s2.0 S0195666314000804 MainDocument12 pagini1 s2.0 S0195666314000804 MainAnonymous 12ikjveo7Încă nu există evaluări
- 270832Document13 pagini270832Anonymous 12ikjveo7Încă nu există evaluări
- Appetite: Rachel Pechey, Pablo Monsivais, Yin-Lam NG, Theresa M. MarteauDocument9 paginiAppetite: Rachel Pechey, Pablo Monsivais, Yin-Lam NG, Theresa M. MarteauAnonymous 12ikjveo7Încă nu există evaluări
- Appetite: Rachel Pechey, Pablo Monsivais, Yin-Lam NG, Theresa M. MarteauDocument9 paginiAppetite: Rachel Pechey, Pablo Monsivais, Yin-Lam NG, Theresa M. MarteauAnonymous 12ikjveo7Încă nu există evaluări
- 98 160 1 SMDocument8 pagini98 160 1 SMAnonymous 12ikjveo7Încă nu există evaluări
- 1 s2.0 S0891524514003575 MainDocument12 pagini1 s2.0 S0891524514003575 MainAnonymous 12ikjveo7Încă nu există evaluări
- Appetite: Rachel Pechey, Pablo Monsivais, Yin-Lam NG, Theresa M. MarteauDocument9 paginiAppetite: Rachel Pechey, Pablo Monsivais, Yin-Lam NG, Theresa M. MarteauAnonymous 12ikjveo7Încă nu există evaluări
- 9305768Document10 pagini9305768Anonymous 12ikjveo7Încă nu există evaluări
- 00 B 4951 C 00 B 7545 F 59000000Document19 pagini00 B 4951 C 00 B 7545 F 59000000Anonymous 12ikjveo7Încă nu există evaluări
- 1 s2.0 S0167629615001368 MainDocument8 pagini1 s2.0 S0167629615001368 MainAnonymous 12ikjveo7Încă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (120)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- EwingDocument10 paginiEwingMd Ahsanuzzaman PinkuÎncă nu există evaluări
- 18 OctDocument82 pagini18 OctAseel AlsheeshÎncă nu există evaluări
- First Aid LeafletDocument11 paginiFirst Aid LeafletshahnawazÎncă nu există evaluări
- 17-9 eJDD FinalDocument100 pagini17-9 eJDD FinalMohamed GamalÎncă nu există evaluări
- Lencastre Et Al-2019-Journal of The European Academy of Dermatology and VenereologyDocument2 paginiLencastre Et Al-2019-Journal of The European Academy of Dermatology and VenereologyMaria MogosÎncă nu există evaluări
- Lumbar Myofascial Pain SyndromeDocument8 paginiLumbar Myofascial Pain SyndromeYani Desi YantiÎncă nu există evaluări
- Topic - Importance of Getting Vaccinated During PandemicDocument3 paginiTopic - Importance of Getting Vaccinated During PandemicRitik BinaniÎncă nu există evaluări
- Syndrome of Inappropriate Vasopressin Sexretion (Siadh)Document22 paginiSyndrome of Inappropriate Vasopressin Sexretion (Siadh)Moni RethÎncă nu există evaluări
- Complex Regional Pain Syndrome (CRPS) : CausesDocument1 paginăComplex Regional Pain Syndrome (CRPS) : CausesMarisa OktavianaÎncă nu există evaluări
- Assignment1-UnaniMedicine Dosage LabellingDocument12 paginiAssignment1-UnaniMedicine Dosage LabellingFarhat JahanÎncă nu există evaluări
- 7 - Toronto Notes 2011 - Diagnostic Medical ImagingDocument32 pagini7 - Toronto Notes 2011 - Diagnostic Medical Imagingqobsar100% (1)
- 162 Dham 8 1999Document6 pagini162 Dham 8 1999Nur Sidiq Agung SÎncă nu există evaluări
- Endodontic Surgery: Incision and DrainageDocument8 paginiEndodontic Surgery: Incision and DrainageHadoo OolaÎncă nu există evaluări
- The Five Commandments of Infectious Disease ControlDocument2 paginiThe Five Commandments of Infectious Disease ControlCarol ReedÎncă nu există evaluări
- Appendix 8 PDQ39 PDFDocument3 paginiAppendix 8 PDQ39 PDFdrrselvarajÎncă nu există evaluări
- NvsDocument49 paginiNvsChong Uy AlawiÎncă nu există evaluări
- Central Neuraxial Blockade: Major ComplicationsDocument26 paginiCentral Neuraxial Blockade: Major ComplicationsGareth SymonsÎncă nu există evaluări
- Nutrition Now 8Th Edition Brown Test Bank Full Chapter PDFDocument39 paginiNutrition Now 8Th Edition Brown Test Bank Full Chapter PDFdaviddulcieagt6100% (10)
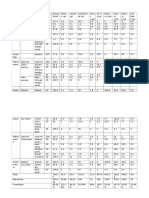
- Tabel JurnalDocument11 paginiTabel JurnalEddy KurniawanÎncă nu există evaluări
- Global and Regional Immunization Profile Global: Population Data in ThousandsDocument1 paginăGlobal and Regional Immunization Profile Global: Population Data in ThousandsAlharis FirmanÎncă nu există evaluări
- Is Marijuana Good or BadDocument3 paginiIs Marijuana Good or BadGenry TanÎncă nu există evaluări
- Mexican Bed BugDocument10 paginiMexican Bed BugPatrick Ross Serquiña DulayÎncă nu există evaluări
- NURSING Review Session (Nur 220) Part 1Document8 paginiNURSING Review Session (Nur 220) Part 1Mariel EstoniloÎncă nu există evaluări
- Cefuroxime Drug StudyDocument4 paginiCefuroxime Drug StudyDona Jane BritosÎncă nu există evaluări
- Heirs of Deauna vs. Fil-Star Maritime Corp.Document31 paginiHeirs of Deauna vs. Fil-Star Maritime Corp.Coleen ReyesÎncă nu există evaluări
- Mini-OSCE Simulation: Hypertensive Disorders in PregnancyDocument16 paginiMini-OSCE Simulation: Hypertensive Disorders in PregnancyNinaÎncă nu există evaluări
- Bingli 1Document5 paginiBingli 1Indah T.IÎncă nu există evaluări
- Morphine SulfateDocument5 paginiMorphine Sulfateapi-3797941100% (4)
- NCP and DrugsDocument13 paginiNCP and DrugsApRil ANn ChUa BingcangÎncă nu există evaluări
- Inserting IV Cannula LessonsDocument3 paginiInserting IV Cannula LessonsAlkenedy KahalÎncă nu există evaluări