S-ar putea să vă placă și
- B MJ AppendicitisDocument6 paginiB MJ AppendicitisXavier QuinteroÎncă nu există evaluări
- Abdominal Burkitt's Lymphoma in ChildrenDocument6 paginiAbdominal Burkitt's Lymphoma in ChildrenNatasya Ryani PurbaÎncă nu există evaluări
- Stress Oxidative and ApoptosisDocument11 paginiStress Oxidative and ApoptosisNatasya Ryani PurbaÎncă nu există evaluări
- Approach To A Case of Hyperuricemia: Singh V, Gomez VV, Swamy SGDocument7 paginiApproach To A Case of Hyperuricemia: Singh V, Gomez VV, Swamy SGsharu4291Încă nu există evaluări
- Histological Wndings of The Internal Inguinal Ring in Patients PDFDocument4 paginiHistological Wndings of The Internal Inguinal Ring in Patients PDFNatasya Ryani PurbaÎncă nu există evaluări
- Abstract Global Prevalence of HyperuricemiaDocument5 paginiAbstract Global Prevalence of HyperuricemiaNatasya Ryani PurbaÎncă nu există evaluări
- Microbiology of Chronic RhinosinusitisDocument10 paginiMicrobiology of Chronic RhinosinusitisNatasya Ryani PurbaÎncă nu există evaluări
- Clin Diabetes 2006 Kruse 91 3Document3 paginiClin Diabetes 2006 Kruse 91 3Natasya Ryani PurbaÎncă nu există evaluări
- Gout in CKDDocument6 paginiGout in CKDNatasya Ryani PurbaÎncă nu există evaluări
- Abstract Global Prevalence of HyperuricemiaDocument5 paginiAbstract Global Prevalence of HyperuricemiaNatasya Ryani PurbaÎncă nu există evaluări
- ON-K5 Cancer PreventionDocument9 paginiON-K5 Cancer PreventionRian AprizaÎncă nu există evaluări
- Rencana Aktivitas PPODocument9 paginiRencana Aktivitas PPONatasya Ryani PurbaÎncă nu există evaluări
- FM - K36 - Prenatal CareDocument33 paginiFM - K36 - Prenatal CareNatasya Ryani PurbaÎncă nu există evaluări
- ONK - K16 - Cervical Cancer (Obgyn)Document49 paginiONK - K16 - Cervical Cancer (Obgyn)Natasya Ryani PurbaÎncă nu există evaluări
- K9 - FKG - Manifestation Systemic DiseaseDocument48 paginiK9 - FKG - Manifestation Systemic DiseaseNatasya Ryani PurbaÎncă nu există evaluări
- Trigeminal Neuralgia1Document28 paginiTrigeminal Neuralgia1Tryyudia R. HalsenÎncă nu există evaluări
- GIS1 - K3 - Histologi Digestive TractDocument49 paginiGIS1 - K3 - Histologi Digestive TractNatasya Ryani Purba100% (1)
- K22 - GIZI - 14 MNT For Stroke 2014 RevisionDocument27 paginiK22 - GIZI - 14 MNT For Stroke 2014 RevisionTrisna Dwi LestariÎncă nu există evaluări
- Gastrointestinal AnatomyDocument70 paginiGastrointestinal AnatomyNatasya Ryani PurbaÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Novo's internationalization strategy through strategic JVs and acquisitionsDocument3 paginiNovo's internationalization strategy through strategic JVs and acquisitionsAbhishek NayakÎncă nu există evaluări
- S02 Dispensing CalculationDocument15 paginiS02 Dispensing CalculationJoe BlackÎncă nu există evaluări
- Effective Home Remedies With HerbsDocument23 paginiEffective Home Remedies With HerbsAlexandru Vasile100% (1)
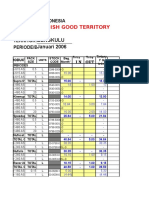
- PT. Makmur Sejahtera Indonesia Persada Daftar Harga Jual BarangDocument28 paginiPT. Makmur Sejahtera Indonesia Persada Daftar Harga Jual BarangIFRSMBÎncă nu există evaluări
- Daftar Formularium Obat di UPT Puskesmas RandulawangDocument7 paginiDaftar Formularium Obat di UPT Puskesmas RandulawangutamiÎncă nu există evaluări
- Pure Steam For Pharmaceutical SterilizersDocument33 paginiPure Steam For Pharmaceutical Sterilizershansenmike698105100% (1)
- InfoDocument438 paginiInfoAakash KumarÎncă nu există evaluări
- 2011 ApmsaDocument302 pagini2011 ApmsaChristopher SchmittÎncă nu există evaluări
- Asia3 Product List 2 PDFDocument17 paginiAsia3 Product List 2 PDFYoussef KaidÎncă nu există evaluări
- Document (12) 1Document7 paginiDocument (12) 1Fazal JalalÎncă nu există evaluări
- 2016 - Text Book of Clinical Pharmacognosy Dr. Mansoor Ahmad Karachi UiversityDocument600 pagini2016 - Text Book of Clinical Pharmacognosy Dr. Mansoor Ahmad Karachi UiversityAmini Mohammad Humayoon100% (1)
- Hyoscine ButylbromideDocument2 paginiHyoscine ButylbromideKepslock StahpÎncă nu există evaluări
- Glycans AplicacionesDocument180 paginiGlycans AplicacionesIvanaColinÎncă nu există evaluări
- Stevens-Johnson Syndrome: Toxic Epidermal NecrolysisDocument21 paginiStevens-Johnson Syndrome: Toxic Epidermal NecrolysisSukiswanti Andryana SariÎncă nu există evaluări
- Biochem Lab 5Document12 paginiBiochem Lab 5Khadijah Ulol AzmiÎncă nu există evaluări
- Failure InvestigationsDocument23 paginiFailure InvestigationsVaishali Kurdikar100% (1)
- Cost - Effective Natural Binder EfficiencyDocument40 paginiCost - Effective Natural Binder EfficiencyYudi GugupÎncă nu există evaluări
- Pepcid Case AnalysisDocument6 paginiPepcid Case AnalysisessÎncă nu există evaluări
- Physical Pharmacy Laboratory Experiment No PDFDocument8 paginiPhysical Pharmacy Laboratory Experiment No PDFAria DomingoÎncă nu există evaluări
- Life of The King - Presentation About Life of Elvis PresleyDocument31 paginiLife of The King - Presentation About Life of Elvis PresleyAlmedin HibićÎncă nu există evaluări
- Food and Drug Interactions A General ReviewDocument15 paginiFood and Drug Interactions A General ReviewDaniela AndreiÎncă nu există evaluări
- Arroz Con Mango PDFDocument197 paginiArroz Con Mango PDFVanshika JainÎncă nu există evaluări
- Survey of The Role of Community Pharmacists in The Management of Tuberculosis in Delta State (Abstract)Document10 paginiSurvey of The Role of Community Pharmacists in The Management of Tuberculosis in Delta State (Abstract)Ichipi-ifukor Patrick ChukuyenumÎncă nu există evaluări
- 2013 Source BookDocument172 pagini2013 Source BookAlex EspinozaÎncă nu există evaluări
- I Hi Trigger Tool For Measuring Adverse Drug EventsDocument16 paginiI Hi Trigger Tool For Measuring Adverse Drug EventsGaby ValenzuelaÎncă nu există evaluări
- Production Scheduling in Pharmaceutical IndustryDocument83 paginiProduction Scheduling in Pharmaceutical IndustrySubhodeep SenguptaÎncă nu există evaluări
- Biopharmaceutical Sales Managed Care in FT Lauderdale West Palm Beach FL Resume Amit GargDocument2 paginiBiopharmaceutical Sales Managed Care in FT Lauderdale West Palm Beach FL Resume Amit GargAmitGarg2Încă nu există evaluări
- History TakingDocument67 paginiHistory TakingOluremi KehindeÎncă nu există evaluări
- Natco PipelineDocument5 paginiNatco Pipelinenikesh.nikzagÎncă nu există evaluări
- Tariq Endo SeminarDocument31 paginiTariq Endo SeminarSayedAbdulMugeesÎncă nu există evaluări