S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Dentsply GAC - CatalogDocument336 paginiDentsply GAC - Catalogsorc50% (2)
- Symposium 2017 Pforzheim en NewDocument28 paginiSymposium 2017 Pforzheim en NewsorcÎncă nu există evaluări
- 6a4 Cements en LowDocument2 pagini6a4 Cements en LowsorcÎncă nu există evaluări
- PDFDocument7 paginiPDFsorcÎncă nu există evaluări
- BrosutaDocument28 paginiBrosutasorcÎncă nu există evaluări
- CCO Patient Diagnostic Sheet v6Document2 paginiCCO Patient Diagnostic Sheet v6sorcÎncă nu există evaluări
- AsdwDocument56 paginiAsdwsorcÎncă nu există evaluări
- New Concepts in Orthodontics, Occlusion and TMJ DysfunctionDocument8 paginiNew Concepts in Orthodontics, Occlusion and TMJ DysfunctionsorcÎncă nu există evaluări
- TMJ 2015 PDFDocument8 paginiTMJ 2015 PDFsorcÎncă nu există evaluări
- The Influence of Cranio-Cervical Posture On Maximal Mouth Opening and Pressure Pain Threshold in Patients With Myofascial Temporomandibular Pain DisordersDocument8 paginiThe Influence of Cranio-Cervical Posture On Maximal Mouth Opening and Pressure Pain Threshold in Patients With Myofascial Temporomandibular Pain DisordersFelipeVidalÎncă nu există evaluări
- TMJ 2015Document8 paginiTMJ 2015sorcÎncă nu există evaluări
- JFLS-20 Item - 2013-05-12Document1 paginăJFLS-20 Item - 2013-05-12sorcÎncă nu există evaluări
- Eng SubjectsDocument25 paginiEng SubjectssorcÎncă nu există evaluări
- New Concepts in Orthodontics, Occlusion and TMJ DysfunctionDocument8 paginiNew Concepts in Orthodontics, Occlusion and TMJ DysfunctionsorcÎncă nu există evaluări
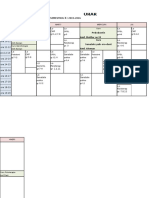
- Orar An 6 MD Seria 1 Sem LL 2015-2016Document2 paginiOrar An 6 MD Seria 1 Sem LL 2015-2016sorcÎncă nu există evaluări
- Spofa Catalogue en 2013 2014Document59 paginiSpofa Catalogue en 2013 2014sorcÎncă nu există evaluări
- In OvationRArticlebyJerryClark IncreasingEfficiencyandProfitwithSelf LigatingBracketsDocument5 paginiIn OvationRArticlebyJerryClark IncreasingEfficiencyandProfitwithSelf LigatingBracketssorcÎncă nu există evaluări
- Over The Last 2 Weeks, How Often Have You Been Bothered by The Following Problems? Place A Check Mark in The Box To Indicate Your AnswerDocument1 paginăOver The Last 2 Weeks, How Often Have You Been Bothered by The Following Problems? Place A Check Mark in The Box To Indicate Your AnswersorcÎncă nu există evaluări
- Patient Health Questionnaire-15: Physical SymptomsDocument1 paginăPatient Health Questionnaire-15: Physical SymptomssorcÎncă nu există evaluări
- Oral Behavior Checklist - 2013!05!12Document1 paginăOral Behavior Checklist - 2013!05!12sorcÎncă nu există evaluări
- CCO Patient Diagnostic Sheet (Breakdown)Document1 paginăCCO Patient Diagnostic Sheet (Breakdown)sorcÎncă nu există evaluări
- Oral Behavior Checklist - 2013!05!12Document1 paginăOral Behavior Checklist - 2013!05!12sorcÎncă nu există evaluări
- Oral Behavior Checklist - 2013!05!12Document1 paginăOral Behavior Checklist - 2013!05!12sorcÎncă nu există evaluări
- Nihms 695420fgdfgDocument40 paginiNihms 695420fgdfgsorcÎncă nu există evaluări
- Graded Chronic Pain v2 - 1 Month - 2013!05!12mnbDocument1 paginăGraded Chronic Pain v2 - 1 Month - 2013!05!12mnbsorcÎncă nu există evaluări
- Nihms 695420fgdfgDocument40 paginiNihms 695420fgdfgsorcÎncă nu există evaluări
- JFLS-20 Item - 2013-05-12Document1 paginăJFLS-20 Item - 2013-05-12sorcÎncă nu există evaluări
- DC-TMD Examform International 2013-05-12Document2 paginiDC-TMD Examform International 2013-05-12sorcÎncă nu există evaluări
- Graded Chronic Pain v2 - 1 Month - 2013!05!12Document1 paginăGraded Chronic Pain v2 - 1 Month - 2013!05!12sorcÎncă nu există evaluări
- Semi Solids PDFDocument3 paginiSemi Solids PDFAsif Hasan NiloyÎncă nu există evaluări
- Introduction To Psychology BrochureDocument2 paginiIntroduction To Psychology BrochureErika JimenezÎncă nu există evaluări
- ManeuversDocument16 paginiManeuversCezar-George BadaleÎncă nu există evaluări
- Investigations For Diseases of The Tongue A Review PDFDocument6 paginiInvestigations For Diseases of The Tongue A Review PDFShantanu DixitÎncă nu există evaluări
- hw410 Unit 9 Assignment Final ProjectDocument9 paginihw410 Unit 9 Assignment Final Projectapi-649875164Încă nu există evaluări
- MHFL Functional FoodsDocument24 paginiMHFL Functional FoodsZekel HealthcareÎncă nu există evaluări
- Sop Cleaning Rev 06 - 2018 Rev Baru (Repaired)Document20 paginiSop Cleaning Rev 06 - 2018 Rev Baru (Repaired)FajarRachmadiÎncă nu există evaluări
- Appointments Boards and Commissions 09-01-15Document23 paginiAppointments Boards and Commissions 09-01-15L. A. PatersonÎncă nu există evaluări
- Radiation Protection 2018Document213 paginiRadiation Protection 2018Ricardo EdanoÎncă nu există evaluări
- Sickle-Cell AnemiaDocument11 paginiSickle-Cell Anemiahalzen_joyÎncă nu există evaluări
- 2017EffectofConsumptionKemuningsLeafMurrayaPaniculataL JackInfusetoReduceBodyMassIndexWaistCircumferenceandPelvisCircumferenceonObesePatientsDocument5 pagini2017EffectofConsumptionKemuningsLeafMurrayaPaniculataL JackInfusetoReduceBodyMassIndexWaistCircumferenceandPelvisCircumferenceonObesePatientsvidianka rembulanÎncă nu există evaluări
- Ancient Indian Medicine Systems OverviewDocument11 paginiAncient Indian Medicine Systems OverviewAmrutha AyinavoluÎncă nu există evaluări
- Csa Fodrea 2014 - 2015 Student Handbook FinalDocument37 paginiCsa Fodrea 2014 - 2015 Student Handbook Finalapi-260407035Încă nu există evaluări
- State Act ListDocument3 paginiState Act Listalkca_lawyer100% (1)
- Senior Counsel or Associate General Counsel or Assistant GeneralDocument3 paginiSenior Counsel or Associate General Counsel or Assistant Generalapi-76922317Încă nu există evaluări
- Manage WHS Operations - Assessment 2 - v8.2Document5 paginiManage WHS Operations - Assessment 2 - v8.2Daniela SanchezÎncă nu există evaluări
- 1 s2.0 S2214785321052202 MainDocument4 pagini1 s2.0 S2214785321052202 MainTusher Kumar SahaÎncă nu există evaluări
- Autismo: Modelos Educativos para Una Vida de Calidad: J. TamaritDocument6 paginiAutismo: Modelos Educativos para Una Vida de Calidad: J. TamaritMonicaJaimesMartinezÎncă nu există evaluări
- Antioxidant and Stability of Dragon Fruit Peel ColourDocument3 paginiAntioxidant and Stability of Dragon Fruit Peel ColourPatricia VellanoÎncă nu există evaluări
- Low Back Pain Dr. Hardhi PRanataDocument57 paginiLow Back Pain Dr. Hardhi PRanataPerwita ArumingtyasÎncă nu există evaluări
- Mumps Guide: Causes, Symptoms, Treatment & PreventionDocument14 paginiMumps Guide: Causes, Symptoms, Treatment & PreventionChristian JonathanÎncă nu există evaluări
- Neonatal LupusDocument19 paginiNeonatal Lupusyogeshraval368Încă nu există evaluări
- Dr. LakshmayyaDocument5 paginiDr. LakshmayyanikhilbÎncă nu există evaluări
- Nabh CleaningDocument6 paginiNabh CleaningArchana GaonkarÎncă nu există evaluări
- 80-Article Text-264-1-10-20200729Document6 pagini80-Article Text-264-1-10-20200729ulfaÎncă nu există evaluări
- Nematode EggsDocument5 paginiNematode EggsEmilia Antonia Salinas TapiaÎncă nu există evaluări
- 7 Millets That Grow in Your Backyard and What You Can Do With ThemDocument16 pagini7 Millets That Grow in Your Backyard and What You Can Do With ThemDevrajÎncă nu există evaluări
- Start and Run Sandwich and Coffee Shops PDFDocument193 paginiStart and Run Sandwich and Coffee Shops PDFsap7e88% (8)
- 15.1 - PH II - Leave Rules-2019Document40 pagini15.1 - PH II - Leave Rules-2019Ranjeet SinghÎncă nu există evaluări
- Turn Around Time of Lab: Consultant Hospital ManagementDocument22 paginiTurn Around Time of Lab: Consultant Hospital ManagementAshok KhandelwalÎncă nu există evaluări