S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- NDA073 New Psychoactive Substances (NPS)Document3 paginiNDA073 New Psychoactive Substances (NPS)Gian Alodia RisamasuÎncă nu există evaluări
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Rheumatic Diseases Presentation GuideDocument24 paginiRheumatic Diseases Presentation GuideGian Alodia RisamasuÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Reccmiss CzEvalTrtDocument13 paginiReccmiss CzEvalTrtGian Alodia RisamasuÎncă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (894)
- Pat's Jurding Word FormatDocument10 paginiPat's Jurding Word FormatGian Alodia RisamasuÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Jurnal PCOSDocument39 paginiJurnal PCOSGian Alodia RisamasuÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- About Brain Injury: Physical Impairments-Speech, Vision, HearingDocument1 paginăAbout Brain Injury: Physical Impairments-Speech, Vision, HearingGian Alodia RisamasuÎncă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Jurnal Alod FixDocument25 paginiJurnal Alod FixGian Alodia RisamasuÎncă nu există evaluări
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- ArticleDocument6 paginiArticleGian Alodia RisamasuÎncă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Blunt Liver Trauma PDFDocument10 paginiBlunt Liver Trauma PDFGian Alodia RisamasuÎncă nu există evaluări
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- Safety of Surgical Treatment of Hemorrhoids in Elderly PatientsDocument6 paginiSafety of Surgical Treatment of Hemorrhoids in Elderly PatientsGian Alodia RisamasuÎncă nu există evaluări
- Review Article: Inflammation, Vasospasm, and Brain Injury After Subarachnoid HemorrhageDocument16 paginiReview Article: Inflammation, Vasospasm, and Brain Injury After Subarachnoid HemorrhageGian Alodia RisamasuÎncă nu există evaluări
- Jurnal 10 - Ganda Sigalingging1Document10 paginiJurnal 10 - Ganda Sigalingging1umamfazlurrahmanÎncă nu există evaluări
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Rolle of Surgery in Oncology: Surgery Departement Medical Faculty Ukrida UniversityDocument25 paginiThe Rolle of Surgery in Oncology: Surgery Departement Medical Faculty Ukrida UniversityGian Alodia RisamasuÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Bicycle Repair ManualDocument162 paginiBicycle Repair Manualrazvancc89% (9)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- A Comparative Study of Different Image Denoising Methods: Afreen Mulla, A.G.Patil, Sneha Pethkar, Nishigandha DeshmukhDocument6 paginiA Comparative Study of Different Image Denoising Methods: Afreen Mulla, A.G.Patil, Sneha Pethkar, Nishigandha DeshmukherpublicationÎncă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Advance Distributed ComputingDocument2 paginiAdvance Distributed ComputingValia Centre of ExcellenceÎncă nu există evaluări
- Sigmund Freud and His Main TheoriesDocument5 paginiSigmund Freud and His Main TheoriesNguyen HarryÎncă nu există evaluări
- Mascot LD series hydraulic motor specsDocument6 paginiMascot LD series hydraulic motor specsM S GokulÎncă nu există evaluări
- 1 Clock Domain CrossingDocument35 pagini1 Clock Domain CrossingRamakrishnaRao SoogooriÎncă nu există evaluări
- QY25K5-I Technical Specifications (SC8DK280Q3)Document11 paginiQY25K5-I Technical Specifications (SC8DK280Q3)Everton Rai Pereira Feireira100% (1)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Examining Language in Romeo and Juliet - The Prologue - Mastery TestDocument5 paginiExamining Language in Romeo and Juliet - The Prologue - Mastery TestPhạm MyÎncă nu există evaluări
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- Introducing The Phenomenon To Be Discussed: Stating Your OpinionDocument8 paginiIntroducing The Phenomenon To Be Discussed: Stating Your OpinionRam RaghuwanshiÎncă nu există evaluări
- Report Card of Army Public School StudentDocument2 paginiReport Card of Army Public School StudentRama KrishnaÎncă nu există evaluări
- Drainage PDFDocument1 paginăDrainage PDFSwapnil JainÎncă nu există evaluări
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- TM-1870 AVEVA Everything3D - (2.1) Draw Administration (CN)Document124 paginiTM-1870 AVEVA Everything3D - (2.1) Draw Administration (CN)yuehui niuÎncă nu există evaluări
- Writing Emails Part 1 Informal British English Teacher Ver2Document7 paginiWriting Emails Part 1 Informal British English Teacher Ver2Madalina MandiucÎncă nu există evaluări
- Ethics in ResearchDocument21 paginiEthics in Researchmukku_raviÎncă nu există evaluări
- Graffiti Model Lesson PlanDocument9 paginiGraffiti Model Lesson Planapi-286619177100% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- CA Ashish Dewani - Resume-1Document2 paginiCA Ashish Dewani - Resume-1Payal JainÎncă nu există evaluări
- Kerala University 2013 Admission ProspectusDocument50 paginiKerala University 2013 Admission ProspectusMuneer SainulabdeenÎncă nu există evaluări
- The Machine-Room-Less Elevator: Kone E MonospaceDocument8 paginiThe Machine-Room-Less Elevator: Kone E MonospaceAbdelmuneimÎncă nu există evaluări
- List of Electronics Manufacturing Companies in Noida - ElectronicsmediaDocument2 paginiList of Electronics Manufacturing Companies in Noida - ElectronicsmediaBlue Oceon50% (4)
- Foundation ProblemsDocument71 paginiFoundation Problemsيقين يقين0% (1)
- PLC SCADA ASSIGNMENT SsDocument10 paginiPLC SCADA ASSIGNMENT SsShadab AhmadÎncă nu există evaluări
- ZSL National Red List of Nepal's Birds Volume 2Document636 paginiZSL National Red List of Nepal's Birds Volume 2Tushita LamaÎncă nu există evaluări
- Module II Lecture 4Document19 paginiModule II Lecture 4Prateek NayakÎncă nu există evaluări
- RMC Case StudyDocument2 paginiRMC Case StudyAmer RahmahÎncă nu există evaluări
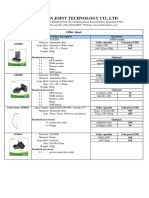
- Vehicle Tracker Offer SheetDocument1 paginăVehicle Tracker Offer SheetBihun PandaÎncă nu există evaluări
- Hardware Devices Used in Virtual Reality TechnologiesDocument6 paginiHardware Devices Used in Virtual Reality TechnologiesTheMoon LightÎncă nu există evaluări
- PC 5400 PC 5500Document53 paginiPC 5400 PC 5500ArturHeiseÎncă nu există evaluări
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Development Drop - Number - Peformance - For - EstimateDocument11 paginiDevelopment Drop - Number - Peformance - For - Estimateanon_459056029Încă nu există evaluări
- Maklumat Vaksinasi: Vaccination DetailsDocument1 paginăMaklumat Vaksinasi: Vaccination Detailsaccung manÎncă nu există evaluări
- Interview QuestionsDocument3 paginiInterview Questionsاحتشام چوہدری100% (1)