S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Benign Thyroid Disorders OkeDocument31 paginiBenign Thyroid Disorders OkeAgatha Billkiss IsmailÎncă nu există evaluări
- Psychogenic Pain 1Document23 paginiPsychogenic Pain 1Agatha Billkiss IsmailÎncă nu există evaluări
- Acute Abdomen and PeritonitisDocument17 paginiAcute Abdomen and PeritonitisAgatha Billkiss IsmailÎncă nu există evaluări
- Power Point KBKDocument105 paginiPower Point KBKangkawinataÎncă nu există evaluări
- Li Et Al-2015-European Journal of ImmunologyDocument11 paginiLi Et Al-2015-European Journal of ImmunologyAgatha Billkiss IsmailÎncă nu există evaluări
- Somatization PDFDocument3 paginiSomatization PDFAgatha Billkiss IsmailÎncă nu există evaluări
- International Headache Classification III ICHD III 2013 Beta 1Document180 paginiInternational Headache Classification III ICHD III 2013 Beta 1Fityan Aulia RahmanÎncă nu există evaluări
- ACG Guideline AcutePancreatitis September 2013Document16 paginiACG Guideline AcutePancreatitis September 2013gorditomaloÎncă nu există evaluări
- Lung Function Iced Saline EditorialDocument2 paginiLung Function Iced Saline EditorialAgatha Billkiss IsmailÎncă nu există evaluări
- Lung Function Iced Saline EditorialDocument2 paginiLung Function Iced Saline EditorialAgatha Billkiss IsmailÎncă nu există evaluări
- Choices in Fluid Type and Volume During Resuscitation Impact On Patient Outcomes PDFDocument13 paginiChoices in Fluid Type and Volume During Resuscitation Impact On Patient Outcomes PDFfbihansipÎncă nu există evaluări
- Fluid Resuscitation in Septic ShockDocument56 paginiFluid Resuscitation in Septic ShockAgatha Billkiss Ismail100% (1)
- Identification of Malassezia SpeciesDocument3 paginiIdentification of Malassezia SpeciesSJ IraaÎncă nu există evaluări
- Mohammad Mobasheri SPR General SurgeryDocument17 paginiMohammad Mobasheri SPR General SurgeryZidnaÎncă nu există evaluări
- Tinea PedisDocument4 paginiTinea PediskirustagyÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Prostate Cancer PDFDocument2 paginiProstate Cancer PDFkapczukÎncă nu există evaluări
- Nursing Care Plans - Nursing Dia - Gulanick, MegDocument1.374 paginiNursing Care Plans - Nursing Dia - Gulanick, Megeric parl91% (22)
- BiologyDocument14 paginiBiologyKanish KumarÎncă nu există evaluări
- MBF7823423Document425 paginiMBF7823423Pete PetersÎncă nu există evaluări
- Pediatric AnesthesiaDocument70 paginiPediatric AnesthesiaEliyan KhanimovÎncă nu există evaluări
- Product RicanatorDocument2 paginiProduct RicanatorSaravanan Kanagavel100% (1)
- Pain Fellowship ProgramDocument14 paginiPain Fellowship ProgramshahidkhattakÎncă nu există evaluări
- Cps-Pg-Admission-2019 First Selection Round of Neet Eligible Candidates For The State of MaharashtraDocument93 paginiCps-Pg-Admission-2019 First Selection Round of Neet Eligible Candidates For The State of MaharashtrarohankananiÎncă nu există evaluări
- PhotodermatosesDocument8 paginiPhotodermatosesIvan KurniadiÎncă nu există evaluări
- Platelet Rich Plasma, A Powerful Tool in DermatologyDocument10 paginiPlatelet Rich Plasma, A Powerful Tool in DermatologyJulian SilitongaÎncă nu există evaluări
- Case Study On LBWDocument43 paginiCase Study On LBWOmotosho Alex50% (2)
- Rachael Stanton Resume Rachael Stanton LVT 1 2Document2 paginiRachael Stanton Resume Rachael Stanton LVT 1 2api-686124613Încă nu există evaluări
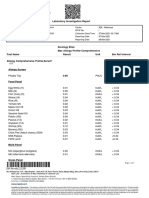
- Laboratory Investigation ReportDocument7 paginiLaboratory Investigation ReportAmarjeetÎncă nu există evaluări
- Aron FinalDocument70 paginiAron FinalJaime Pastrana Jr.Încă nu există evaluări
- GMU Immunization FormDocument5 paginiGMU Immunization FormAurora Kitt McGowanÎncă nu există evaluări
- Isid Guide Ipc in The Radiology DepartmentDocument24 paginiIsid Guide Ipc in The Radiology DepartmentYennitaSatumalayÎncă nu există evaluări
- The Cracked Mirror, Karen KernbergDocument10 paginiThe Cracked Mirror, Karen Kernbergjuaromer100% (1)
- Physics With Illustrative Examples From Medicine and BiologyDocument1 paginăPhysics With Illustrative Examples From Medicine and BiologySivaranjaniÎncă nu există evaluări
- MDOC Sued For Handling of CoronavirusDocument56 paginiMDOC Sued For Handling of CoronavirusTaylor DesOrmeau100% (1)
- Down Screen Proposal For Health Screen at Thyrocare AmitDocument19 paginiDown Screen Proposal For Health Screen at Thyrocare AmitSwatiSuranaÎncă nu există evaluări
- Final Draft of Nursing PhilosophyDocument6 paginiFinal Draft of Nursing Philosophyapi-534634416Încă nu există evaluări
- Essentials of Diagnosis, Treatment, and Application of Cardiac and Peripheral Vascular DiseasesDocument295 paginiEssentials of Diagnosis, Treatment, and Application of Cardiac and Peripheral Vascular DiseasesMichael BrunetÎncă nu există evaluări
- Powerpoint TaeniasisDocument23 paginiPowerpoint TaeniasisAyshaShariff0% (1)
- PolytraumaDocument38 paginiPolytraumarvajrapuÎncă nu există evaluări
- Clinical Notebook A Quick Mnemonic For Predicting Pressure Sores in ED PatientsDocument2 paginiClinical Notebook A Quick Mnemonic For Predicting Pressure Sores in ED PatientsChantal CarnesÎncă nu există evaluări
- Press Release On COVIDEXDocument2 paginiPress Release On COVIDEXNasasira BensonÎncă nu există evaluări
- JednjakDocument15 paginiJednjakbojana1994Încă nu există evaluări
- 01-2020 - Tactical Emergency Casualty Care (TECC)Document5 pagini01-2020 - Tactical Emergency Casualty Care (TECC)pibulinÎncă nu există evaluări
- Daftar PustakaDocument2 paginiDaftar PustakaErick PrasetyaÎncă nu există evaluări
- Health Checklist: NG:) Lumunok)Document2 paginiHealth Checklist: NG:) Lumunok)Rose Duron GumaÎncă nu există evaluări