S-ar putea să vă placă și
- Focused Medical InterviewDocument2 paginiFocused Medical InterviewAlexÎncă nu există evaluări
- CC Concept MapDocument11 paginiCC Concept Mapapi-546355187Încă nu există evaluări
- Pediatric NotesDocument20 paginiPediatric Notestweet196% (23)
- UMMP Guidelines For ExaminationDocument28 paginiUMMP Guidelines For ExaminationayuniÎncă nu există evaluări
- UMMP Guidelines For ExaminationDocument28 paginiUMMP Guidelines For ExaminationayuniÎncă nu există evaluări
- 13-Mike Engelbrecht - Methods of Maintenance On High Voltage Fluid FilledDocument5 pagini13-Mike Engelbrecht - Methods of Maintenance On High Voltage Fluid FilledRomany AllamÎncă nu există evaluări
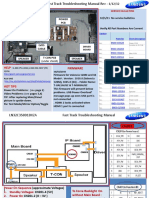
- Samsung LN55C610N1FXZA Fast Track Guide (SM)Document4 paginiSamsung LN55C610N1FXZA Fast Track Guide (SM)Carlos OdilonÎncă nu există evaluări
- Neurology Exam Checklist1Document6 paginiNeurology Exam Checklist1Syed AfzalÎncă nu există evaluări
- Nclex NeuroDocument12 paginiNclex Neuromonmon100% (1)
- (Ob1) 1.02 - History and Physical Exam - Dr. NicanorDocument7 pagini(Ob1) 1.02 - History and Physical Exam - Dr. NicanorJakeÎncă nu există evaluări
- Clinical Scenario and Worksheet For Diagnostic Appraisal (Journal On Dengue)Document3 paginiClinical Scenario and Worksheet For Diagnostic Appraisal (Journal On Dengue)Stephie E.Încă nu există evaluări
- Interview Pa Tool.Document5 paginiInterview Pa Tool.Raisah Bint AbdullahÎncă nu există evaluări
- General AppearanceDocument3 paginiGeneral AppearancePhuong TranÎncă nu există evaluări
- Geriatric Depression ScaleDocument3 paginiGeriatric Depression ScalerejotanganÎncă nu există evaluări
- Clock Drawing TestDocument3 paginiClock Drawing TestNeny PatrowÎncă nu există evaluări
- IM AdconDocument28 paginiIM AdconCla SantosÎncă nu există evaluări
- The Detailed Neurologic Examination in Adults - UpToDate PDFDocument29 paginiThe Detailed Neurologic Examination in Adults - UpToDate PDFMiguel GarciaÎncă nu există evaluări
- Pharmacology Nursing Final ExamDocument103 paginiPharmacology Nursing Final Examkinyuaboris990Încă nu există evaluări
- Acute TonsillitisDocument7 paginiAcute TonsillitisMichael HostiadiÎncă nu există evaluări
- Health HistoryDocument19 paginiHealth HistoryAngelene Caliva100% (1)
- Physical ExaminationDocument7 paginiPhysical ExaminationErwin MirandaÎncă nu există evaluări
- The Cornell Scale For Depression in DementiaDocument12 paginiThe Cornell Scale For Depression in DementiaPopa NiculinaÎncă nu există evaluări
- Head To Toe Checklist (Masroni)Document13 paginiHead To Toe Checklist (Masroni)hillary elsaÎncă nu există evaluări
- Instrumental Activities of Daily Living ScaleDocument1 paginăInstrumental Activities of Daily Living ScaleAnonymous uWlv9rllaÎncă nu există evaluări
- Clinical CasesDocument12 paginiClinical CasesAndreea HanuÎncă nu există evaluări
- Inflamatory Bowel Disease: Dr. Samir IsmailDocument82 paginiInflamatory Bowel Disease: Dr. Samir IsmailGhadeer EbraheemÎncă nu există evaluări
- A Case Presentation - PediaDocument50 paginiA Case Presentation - PediaCathy ChiongÎncă nu există evaluări
- Medicine1 Grand PE ScriptDocument10 paginiMedicine1 Grand PE ScriptCarmeline Santi BeronillaÎncă nu există evaluări
- Rashes in Children by Dr. Muhammad - RashidDocument43 paginiRashes in Children by Dr. Muhammad - RashidAli DkaliÎncă nu există evaluări
- Ob-Gyne: Obstetric History and PEDocument6 paginiOb-Gyne: Obstetric History and PEPorori BookshopÎncă nu există evaluări
- NursingBedsideSwallowingScreen PDFDocument1 paginăNursingBedsideSwallowingScreen PDFLUCASÎncă nu există evaluări
- Infra-Auricular Mass Case PresDocument8 paginiInfra-Auricular Mass Case PresEjay Jacob RicamaraÎncă nu există evaluări
- Comprehensive Adult Health HistoryDocument7 paginiComprehensive Adult Health HistoryKhirsna PasajolÎncă nu există evaluări
- College of Nursing: Drug StudyDocument7 paginiCollege of Nursing: Drug StudyStephen VillegasÎncă nu există evaluări
- Guidelines For The Management of Paracetamol OverdoseDocument1 paginăGuidelines For The Management of Paracetamol Overdoseps_ares2Încă nu există evaluări
- AhafinalheadtoeDocument4 paginiAhafinalheadtoeapi-620081868Încă nu există evaluări
- Pedia CaseDocument65 paginiPedia CaseJason MirasolÎncă nu există evaluări
- PATIENT 1 Nursing Assessment FormDocument5 paginiPATIENT 1 Nursing Assessment FormndemboloveÎncă nu există evaluări
- Normal Adult Lab Values Blood GasesDocument1 paginăNormal Adult Lab Values Blood Gasesmenickel3Încă nu există evaluări
- Acute Hypertension-Hypertensive Urgency and Hypertensive EmergencyDocument13 paginiAcute Hypertension-Hypertensive Urgency and Hypertensive EmergencyAmitKumarÎncă nu există evaluări
- Need Motivates The Behaviour of A Person.: Human Needs TheoryDocument8 paginiNeed Motivates The Behaviour of A Person.: Human Needs TheoryDan Ataniel EnsaladaÎncă nu există evaluări
- Pediatric Initial Patient HistoryDocument11 paginiPediatric Initial Patient HistoryLinh TrịnhÎncă nu există evaluări
- Physical ExamDocument14 paginiPhysical ExamAl Ge IrÎncă nu există evaluări
- Assessment and Concept Map Care Plan: Joseph GorospeDocument5 paginiAssessment and Concept Map Care Plan: Joseph Gorospeapi-497389977Încă nu există evaluări
- ThalassemiaDocument13 paginiThalassemiaMukhlisul AmalÎncă nu există evaluări
- Catatonia Kaplan PDFDocument3 paginiCatatonia Kaplan PDFJuan Sebastian LozanoÎncă nu există evaluări
- Feeding PDF Feeding History QuesDocument8 paginiFeeding PDF Feeding History QuesSophia DaniilÎncă nu există evaluări
- Dams - DVT (New)Document48 paginiDams - DVT (New)Msd KishorÎncă nu există evaluări
- Complete Normal Physical Exam PDFDocument3 paginiComplete Normal Physical Exam PDFFrancisco Casio MataÎncă nu există evaluări
- Physical AssessmentDocument2 paginiPhysical AssessmentFeyd1972Încă nu există evaluări
- Laboratory - Medicine - The - Diagnosis - of - Disease - in - The - Clinical - Laboratory (1) - Páginas-350-370Document21 paginiLaboratory - Medicine - The - Diagnosis - of - Disease - in - The - Clinical - Laboratory (1) - Páginas-350-370Jack Morales MoriÎncă nu există evaluări
- Allergic Rhinitis - University of MichiganDocument12 paginiAllergic Rhinitis - University of MichiganarsyiadlinaÎncă nu există evaluări
- Insulin Therapy in Type 2 Diabetes MellitusDocument40 paginiInsulin Therapy in Type 2 Diabetes MellitusEDWIN WIJAYAÎncă nu există evaluări
- Medical History Outline-2020Document9 paginiMedical History Outline-2020sumiti_kumarÎncă nu există evaluări
- Approach To The Child With Anemia - UpToDateDocument41 paginiApproach To The Child With Anemia - UpToDateDaniel Enrique CardenasÎncă nu există evaluări
- EATING DISORDERS: Note Taking OutlineDocument6 paginiEATING DISORDERS: Note Taking OutlinePaula GarciaÎncă nu există evaluări
- NIH Stroke ScaleDocument7 paginiNIH Stroke ScaleSofia YunitaÎncă nu există evaluări
- Classification of The Epilepsies: Purpose: For Clinical DiagnosisDocument25 paginiClassification of The Epilepsies: Purpose: For Clinical Diagnosisayu rifqiÎncă nu există evaluări
- Gordons Case Pres 1Document5 paginiGordons Case Pres 1JM Asentista0% (1)
- Meningitis-Malaria E PDFDocument44 paginiMeningitis-Malaria E PDFSana ShafeeqÎncă nu există evaluări
- PSGNDocument23 paginiPSGNalpha mae beltranÎncă nu există evaluări
- Comprehensive H&PDocument2 paginiComprehensive H&PjwwisnerÎncă nu există evaluări
- Patient Education ToolkitDocument15 paginiPatient Education ToolkitI Nyoman Gede SemarajanaÎncă nu există evaluări
- Study Guide #10 With HEENT ChecklistDocument4 paginiStudy Guide #10 With HEENT ChecklistPrince DuÎncă nu există evaluări
- Ventricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsDe la EverandVentricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsÎncă nu există evaluări
- Urological History TakingDocument6 paginiUrological History TakingayuniÎncă nu există evaluări
- LP CounsellingDocument1 paginăLP CounsellingayuniÎncă nu există evaluări
- Chest X RAY: Airway and MediastinumDocument2 paginiChest X RAY: Airway and MediastinumayuniÎncă nu există evaluări
- Age CounsellingDocument4 paginiAge CounsellingayuniÎncă nu există evaluări
- PBL Trigger 8.8Document9 paginiPBL Trigger 8.8ayuniÎncă nu există evaluări
- Updated Timetable PDFDocument1 paginăUpdated Timetable PDFayuniÎncă nu există evaluări
- Child at Risk Nov 2016Document16 paginiChild at Risk Nov 2016ayuniÎncă nu există evaluări
- Case Presentation Marking Sheet Surgery PDFDocument1 paginăCase Presentation Marking Sheet Surgery PDFayuniÎncă nu există evaluări
- Dysmorphic Syndromes - Thong Meow KeongDocument53 paginiDysmorphic Syndromes - Thong Meow KeongayuniÎncă nu există evaluări
- History Taking and Examination Technique in ObstetricsDocument52 paginiHistory Taking and Examination Technique in ObstetricsIshak IzharÎncă nu există evaluări
- Lung Cancer Staging Poster UpdatedDocument2 paginiLung Cancer Staging Poster UpdatedCarlos Eduardo Avila100% (1)
- NAC Medications Chart 2016 A2Document1 paginăNAC Medications Chart 2016 A2ayuniÎncă nu există evaluări
- Anaemia in ChildrenDocument53 paginiAnaemia in ChildrenayuniÎncă nu există evaluări
- PPD DR YungDocument1 paginăPPD DR YungayuniÎncă nu există evaluări
- History Taking and Examination Technique in ObstetricsDocument52 paginiHistory Taking and Examination Technique in ObstetricsIshak IzharÎncă nu există evaluări
- Attitude Evaluation Form - 30august2017Document1 paginăAttitude Evaluation Form - 30august2017ayuniÎncă nu există evaluări
- CPG Management of Atrial Fibrillation PDFDocument119 paginiCPG Management of Atrial Fibrillation PDFZee YongÎncă nu există evaluări
- Course - UMMP3107 Bioimaging WeekDocument1 paginăCourse - UMMP3107 Bioimaging WeekayuniÎncă nu există evaluări
- C2014 Posting G Surgery Schedule v2Document8 paginiC2014 Posting G Surgery Schedule v2ayuniÎncă nu există evaluări
- Case Presentation Marking Sheet Surgery PDFDocument1 paginăCase Presentation Marking Sheet Surgery PDFayuniÎncă nu există evaluări
- Procedural Skill Printout SurgeryDocument3 paginiProcedural Skill Printout SurgeryayuniÎncă nu există evaluări
- EOP QuestionsDocument2 paginiEOP QuestionsayuniÎncă nu există evaluări
- ArteriesDocument2 paginiArteriesayuniÎncă nu există evaluări
- Attitude Evaluation For Stage 3.1Document1 paginăAttitude Evaluation For Stage 3.1ayuniÎncă nu există evaluări
- AppendicitisDocument11 paginiAppendicitisayuniÎncă nu există evaluări
- Reflective EssayDocument1 paginăReflective EssayayuniÎncă nu există evaluări
- Case PresentationDocument1 paginăCase PresentationayuniÎncă nu există evaluări
- Report Text The Duck Billed Platypus: (Ornithorhynchus Anatinus)Document2 paginiReport Text The Duck Billed Platypus: (Ornithorhynchus Anatinus)Lilis IndriyaniÎncă nu există evaluări
- A Child With Fever and Hemorrhagic RashDocument3 paginiA Child With Fever and Hemorrhagic RashCynthia GÎncă nu există evaluări
- Grief and BereavementDocument4 paginiGrief and BereavementhaminpocketÎncă nu există evaluări
- Technical EnglishDocument7 paginiTechnical EnglishGul HaiderÎncă nu există evaluări
- User Manual For Scanbox Ergo & Banquet Line: Ambient (Neutral), Hot and Active Cooling. Scanbox Meal Delivery CartsDocument8 paginiUser Manual For Scanbox Ergo & Banquet Line: Ambient (Neutral), Hot and Active Cooling. Scanbox Meal Delivery CartsManunoghiÎncă nu există evaluări
- List of ErpDocument2 paginiList of Erpnavyug vidyapeeth trust mahadÎncă nu există evaluări
- PTPL Ir 2018Document383 paginiPTPL Ir 2018Guan WenhaiÎncă nu există evaluări
- Wayne A. Thorp - Analyzing Supply & Demand Using Point & Figure Charts PDFDocument5 paginiWayne A. Thorp - Analyzing Supply & Demand Using Point & Figure Charts PDFSrinivasÎncă nu există evaluări
- Listening 3b Skills Test 1aDocument3 paginiListening 3b Skills Test 1aPticaSelicaÎncă nu există evaluări
- Term Paper - 2022964Document17 paginiTerm Paper - 2022964Md. Ahbab HasanÎncă nu există evaluări
- A Review of The Mental Workload LiteratureDocument36 paginiA Review of The Mental Workload LiteratureArlene LaguaÎncă nu există evaluări
- E650E650M-17 Guía Estándar para El Montaje de Sensores Piezoeléctricos de Emisión Acústica1Document4 paginiE650E650M-17 Guía Estándar para El Montaje de Sensores Piezoeléctricos de Emisión Acústica1fredy lopezÎncă nu există evaluări
- Xiaopan OS: DescriptionDocument1 paginăXiaopan OS: DescriptionMan SavliÎncă nu există evaluări
- Daftar PustakaDocument1 paginăDaftar PustakaUlul Azmi Rumalutur NeinaÎncă nu există evaluări
- UntitledDocument45 paginiUntitledjemÎncă nu există evaluări
- Assessment 3 Comparative Analysis Primary Vs Secondary SourcesDocument5 paginiAssessment 3 Comparative Analysis Primary Vs Secondary SourcesMATOZA, YLJOE V.Încă nu există evaluări
- Al-Ahbash Evolution and BeliefsDocument4 paginiAl-Ahbash Evolution and BeliefskaptenzainalÎncă nu există evaluări
- PGT Computer Science Kendriya Vidyalaya Entrance Exam Question PapersDocument117 paginiPGT Computer Science Kendriya Vidyalaya Entrance Exam Question PapersimshwezÎncă nu există evaluări
- Future Scope and ConclusionDocument13 paginiFuture Scope and ConclusionGourab PalÎncă nu există evaluări
- Akira 007Document70 paginiAkira 007Ocre OcreÎncă nu există evaluări
- Purchase Spec. For Bar (SB425)Document4 paginiPurchase Spec. For Bar (SB425)Daison PaulÎncă nu există evaluări
- Number SystemsDocument25 paginiNumber SystemsMehwish BilalÎncă nu există evaluări
- Itf EssayDocument18 paginiItf EssayTharshiÎncă nu există evaluări
- Research PaperDocument14 paginiResearch PaperNeil Jhon HubillaÎncă nu există evaluări
- Healthy Body CompositionDocument18 paginiHealthy Body CompositionSDasdaDsadsaÎncă nu există evaluări
- CATL 34189-20AH Low Temperature Cell SpecificationDocument17 paginiCATL 34189-20AH Low Temperature Cell Specificationxueziying741Încă nu există evaluări
- Shaira Narrative Report (Final)Document7 paginiShaira Narrative Report (Final)Sheryll TamangÎncă nu există evaluări
- What Is StevedoringDocument10 paginiWhat Is StevedoringMinhaj KmÎncă nu există evaluări