S-ar putea să vă placă și
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Wilson - Cranial NervesDocument243 paginiWilson - Cranial NervesBiblioteca CSNT100% (13)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Laban - Sub Kamal Salman Mahmoud Jaber Mustafa: Done byDocument40 paginiLaban - Sub Kamal Salman Mahmoud Jaber Mustafa: Done byKool Kaish100% (1)
- Growth and Development of Cranial and Facial RegionDocument81 paginiGrowth and Development of Cranial and Facial RegionSwati PawarÎncă nu există evaluări
- The Muscles of Facial ExpressionDocument14 paginiThe Muscles of Facial ExpressionKarina Ramsingh100% (1)
- Cholesteatoma Part 5 Congenital Cholesteatoma PDFDocument4 paginiCholesteatoma Part 5 Congenital Cholesteatoma PDFSuprit Sn100% (1)
- Surgery Papillary Thyroid CADocument15 paginiSurgery Papillary Thyroid CAMelissa LabadorÎncă nu există evaluări
- Mandible FinalDocument105 paginiMandible FinalErly Berlianda100% (1)
- Patrick J. Willems - Genetic Hearing Loss (2004, Marcel Dekker) PDFDocument500 paginiPatrick J. Willems - Genetic Hearing Loss (2004, Marcel Dekker) PDFCarmen-BadeaÎncă nu există evaluări
- A Case Report On - A Rare Case of Laryngocele in A Young Male MenDocument4 paginiA Case Report On - A Rare Case of Laryngocele in A Young Male MenIOSRjournalÎncă nu există evaluări
- Anatomy of Trigeminal Nerve & Trigeminal Neuralgia: Presented By: DR - Vansh Vardhan Madahar PG1 YearDocument47 paginiAnatomy of Trigeminal Nerve & Trigeminal Neuralgia: Presented By: DR - Vansh Vardhan Madahar PG1 YearVansh Vardhan MadaharÎncă nu există evaluări
- Airway Anatomy & Airway Equipment: Presenter - DR Savita SR - DR Faisal Moderator-Dr ShalviDocument48 paginiAirway Anatomy & Airway Equipment: Presenter - DR Savita SR - DR Faisal Moderator-Dr ShalvilakhwinderÎncă nu există evaluări
- Orthodontics 2 Lec M1 M2Document18 paginiOrthodontics 2 Lec M1 M2bambam1aÎncă nu există evaluări
- Antero Lateral RegionDocument13 paginiAntero Lateral RegionNoemi Nagy-CicealăÎncă nu există evaluări
- Physical Description NiceDocument3 paginiPhysical Description NiceROXANA QUISPE CUADROSÎncă nu există evaluări
- Assessment of The Ear and Hearing AcuityDocument3 paginiAssessment of The Ear and Hearing AcuityJay Debby RuizoÎncă nu există evaluări
- Spear 2008Document9 paginiSpear 2008IlseÎncă nu există evaluări
- Material Adjective in Describing Characteristic and QualityDocument2 paginiMaterial Adjective in Describing Characteristic and QualityAyu Ray Govinda DasiÎncă nu există evaluări
- Cleft Lip and PalateDocument25 paginiCleft Lip and PalateRahul Dhaker100% (1)
- Treacher Collins Syndrome: A Case StudyDocument8 paginiTreacher Collins Syndrome: A Case StudyjoeÎncă nu există evaluări
- Daftar Pustaka KBDocument3 paginiDaftar Pustaka KBYogi OktiandiÎncă nu există evaluări
- Ophthalmic RecordDocument7 paginiOphthalmic RecordandrirombeÎncă nu există evaluări
- Biologic Width Around One - and Two-Piece Titanium ImplantsDocument13 paginiBiologic Width Around One - and Two-Piece Titanium Implantsptrjn_vdc100% (1)
- The EarDocument67 paginiThe EarNathanÎncă nu există evaluări
- Nasopharyngeal Swab Test ChecklistDocument3 paginiNasopharyngeal Swab Test ChecklistNoronisa D. CabugatanÎncă nu există evaluări
- Surgical Anatomy of The Ligamentous Attachments in The Temple and Periorbital Regions (2000)Document17 paginiSurgical Anatomy of The Ligamentous Attachments in The Temple and Periorbital Regions (2000)enzoÎncă nu există evaluări
- HyperthyroidismDocument12 paginiHyperthyroidismShoppe 'n ShoppersÎncă nu există evaluări
- Anatomic Variants and Artefacts in Non Enhanced MRDocument8 paginiAnatomic Variants and Artefacts in Non Enhanced MRlouloupavelÎncă nu există evaluări
- AnatomiaDocument156 paginiAnatomiaNata1511Încă nu există evaluări
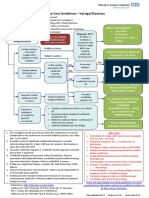
- ENT Vertigo FINAL v0.41Document1 paginăENT Vertigo FINAL v0.41Farmasi BhamadaÎncă nu există evaluări
- Hearing PresentationDocument27 paginiHearing PresentationTaremwa PeterÎncă nu există evaluări