S-ar putea să vă placă și
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Cause: Lymphatic System Oriental Rat Flea Human Flea Septicemic PlagueDocument3 paginiCause: Lymphatic System Oriental Rat Flea Human Flea Septicemic PlagueMattÎncă nu există evaluări
- InfographicDocument1 paginăInfographicapi-531208347Încă nu există evaluări
- Responsible Use of Antibiotics in PoultryDocument24 paginiResponsible Use of Antibiotics in PoultryAbubakar Tahir Ramay100% (1)
- Veterinary Social Work Practice Within Veterinary SettingsDocument13 paginiVeterinary Social Work Practice Within Veterinary SettingsChristopherÎncă nu există evaluări
- One Health Approach: Saving Lives by Taking ADocument4 paginiOne Health Approach: Saving Lives by Taking AagneselimÎncă nu există evaluări
- Question Bank ZoonosisDocument32 paginiQuestion Bank ZoonosisRamesh BeniwalÎncă nu există evaluări
- VeterinaryDocument5 paginiVeterinaryMuhammad A HossainÎncă nu există evaluări
- Dengue Control Starts at HomeDocument1 paginăDengue Control Starts at HomeAlyann Franzen Ardiente OquendoÎncă nu există evaluări
- Event-Based Surveillance Form - 20171229Document6 paginiEvent-Based Surveillance Form - 20171229Activity ManagerÎncă nu există evaluări
- Y8 Biology Worksheet Task 1,2 and 3 SerenaDocument3 paginiY8 Biology Worksheet Task 1,2 and 3 SerenaSERENA TAYÎncă nu există evaluări
- Notes Pack 11.1Document4 paginiNotes Pack 11.1diahemaÎncă nu există evaluări
- Research Paper 1 1Document3 paginiResearch Paper 1 1api-665784764Încă nu există evaluări
- Fvma Student Certification - Application and Skills ValidationDocument14 paginiFvma Student Certification - Application and Skills Validationapi-325687960Încă nu există evaluări
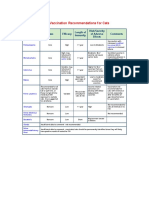
- AVMA Vaccination Recommendations F or CatsDocument2 paginiAVMA Vaccination Recommendations F or CatsHazim Azmi Al-QadryÎncă nu există evaluări
- Microbiology Chapter 17 Spring 07Document3 paginiMicrobiology Chapter 17 Spring 07fallingupward312Încă nu există evaluări
- Summary Profile For Enzootic Bovine Leukosis (Ebl) : Vetsurveillance@defra - Gsi.gov - UkDocument2 paginiSummary Profile For Enzootic Bovine Leukosis (Ebl) : Vetsurveillance@defra - Gsi.gov - UkEnnur NufianÎncă nu există evaluări
- Pertussis or Whooping Cough PowerpointDocument21 paginiPertussis or Whooping Cough PowerpointJay Pee100% (1)
- Typhoid Fever PathophysiologyDocument1 paginăTyphoid Fever PathophysiologyJim Christian EllaserÎncă nu există evaluări
- CSU DVM Term Textbooks FallDocument10 paginiCSU DVM Term Textbooks FallsparkltangrineÎncă nu există evaluări
- 10 Reporting Formats HP Oct2017Document65 pagini10 Reporting Formats HP Oct2017Devendra Singh Tomar100% (1)
- Bird Flu (Avian Influenza)Document6 paginiBird Flu (Avian Influenza)JagadeeshTJÎncă nu există evaluări
- ICAR Accreditation List 2022Document29 paginiICAR Accreditation List 2022Jiliksweta KalitaÎncă nu există evaluări
- Introduction On The Selected OrganizationDocument15 paginiIntroduction On The Selected OrganizationMila K SivanesanÎncă nu există evaluări
- Tetanus Immunity: Understanding Active and Passive ImmunizationDocument12 paginiTetanus Immunity: Understanding Active and Passive ImmunizationRahmatul YasiroÎncă nu există evaluări
- Artikel Kesehatan Dalam Bahasa Inggris Dan Terjemahannya TerbaruDocument3 paginiArtikel Kesehatan Dalam Bahasa Inggris Dan Terjemahannya TerbaruRafaelDimasRizky67% (3)
- Mosquito Borne DiseasesDocument31 paginiMosquito Borne DiseasesRizna SaidÎncă nu există evaluări
- Epidemiologi Kejadian Demam Berdarah Dengue Di Kota Ternate. Maluku UtaraDocument9 paginiEpidemiologi Kejadian Demam Berdarah Dengue Di Kota Ternate. Maluku Utaranur yantiÎncă nu există evaluări
- Practical Manual On Veterinary Clinical Diagnostic Approach 2157 7579 1000337Document10 paginiPractical Manual On Veterinary Clinical Diagnostic Approach 2157 7579 1000337Shravankumar Gaddi100% (1)
- DT ImunisasiDocument54 paginiDT ImunisasiMar'aturrahmahÎncă nu există evaluări
- Veterinary Medicine 08-2016 Room AssignmentDocument7 paginiVeterinary Medicine 08-2016 Room AssignmentPRC BaguioÎncă nu există evaluări