S-ar putea să vă placă și
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- PsychopharmacologyDocument30 paginiPsychopharmacologyHilma Nadhifa100% (1)
- KCC Emergency High Angle DrillDocument18 paginiKCC Emergency High Angle DrillSandy M. MaddaganÎncă nu există evaluări
- Admission and DischargeDocument61 paginiAdmission and DischargeRafia Khalil100% (2)
- KATH - DCH Treatment GuidelinesDocument173 paginiKATH - DCH Treatment GuidelinesCarterine ListÎncă nu există evaluări
- ORTHOSIS - and ProthesisDocument112 paginiORTHOSIS - and Prothesismanjukumard2007100% (1)
- Aquilion ONE GENESIS Edition Transforming CTDocument40 paginiAquilion ONE GENESIS Edition Transforming CTSemeeeJuniorÎncă nu există evaluări
- Atropine Drug StudyDocument3 paginiAtropine Drug StudyMaej83% (6)
- Drug Study ZiprasidoneDocument2 paginiDrug Study ZiprasidoneArnzz Agbulos100% (1)
- Perforative PeritonitisDocument58 paginiPerforative PeritonitisSangeeta BSR82% (17)
- Hospital Review 2017Document32 paginiHospital Review 2017NM Atif100% (5)
- KELOMPOK 1 - RS2 - PRAKTIK BAHASA INGGRIS DetailDocument12 paginiKELOMPOK 1 - RS2 - PRAKTIK BAHASA INGGRIS Detailseren agathaÎncă nu există evaluări
- Hospital PlanningDocument24 paginiHospital PlanningDees_24Încă nu există evaluări
- Issues PPT JbarcoDocument10 paginiIssues PPT Jbarcoapi-654109722Încă nu există evaluări
- Brittany 2Document4 paginiBrittany 2Sharon Williams75% (4)
- Comprehension Book Grade 12Document66 paginiComprehension Book Grade 12milkovicius0% (3)
- Desired Over HaveDocument14 paginiDesired Over HaveJamie LeeÎncă nu există evaluări
- Ayurveda 2nd AnnexureDocument74 paginiAyurveda 2nd AnnexureSmita SaxenaÎncă nu există evaluări
- Essentials of Physiotherapy After Thoracic Surgery - What Physiotherapists Need To Know. A Narrative ReviewDocument15 paginiEssentials of Physiotherapy After Thoracic Surgery - What Physiotherapists Need To Know. A Narrative ReviewMariana MadridÎncă nu există evaluări
- Kugel PDFDocument260 paginiKugel PDFUsman SanaÎncă nu există evaluări
- Chest TraumaDocument39 paginiChest TraumaQuinnee VallejosÎncă nu există evaluări
- KyphosisDocument4 paginiKyphosisclubsanatateÎncă nu există evaluări
- Dlau LVN Resume 1Document1 paginăDlau LVN Resume 1api-571772305Încă nu există evaluări
- Disseminated Intravascular Coagulopathy Dic 1 1Document25 paginiDisseminated Intravascular Coagulopathy Dic 1 1api-394684626Încă nu există evaluări
- Iliotibial Band Syndrome - FannyDocument13 paginiIliotibial Band Syndrome - FannyAlfiani Rosyida Arisanti Syafi'iÎncă nu există evaluări
- Foreign Body of Air PassageDocument19 paginiForeign Body of Air PassageNurul Syazwani RamliÎncă nu există evaluări
- Strickland PresentationDocument1 paginăStrickland Presentationmariopi2495Încă nu există evaluări
- Barodontalgia As A Differential Diagnosis PDFDocument4 paginiBarodontalgia As A Differential Diagnosis PDFDavid ColonÎncă nu există evaluări
- Bedside ClinicDocument6 paginiBedside Clinicyer tagalajÎncă nu există evaluări
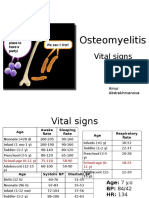
- PBL 2 - OsteomyelitisDocument10 paginiPBL 2 - OsteomyelitisAinur AbdrakhmanovaÎncă nu există evaluări
- Eye Path12Document45 paginiEye Path12JillKellyÎncă nu există evaluări