S-ar putea să vă placă și
- Medical Reiumbursement Software .Document8 paginiMedical Reiumbursement Software .krish104411Încă nu există evaluări
- Personal Details Documents To Be Enclosed: Medical Reiumbursement For State Government EmployeesDocument26 paginiPersonal Details Documents To Be Enclosed: Medical Reiumbursement For State Government EmployeesgsreddyÎncă nu există evaluări
- SHIFWDocument3 paginiSHIFWmandawa786Încă nu există evaluări
- SHIFW (Full Form)Document3 paginiSHIFW (Full Form)harsh dutt vardhanÎncă nu există evaluări
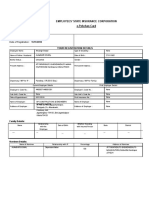
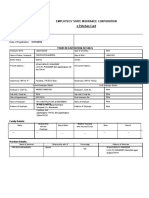
- Employees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationDocument3 paginiEmployees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationRakesh Kumar MohantyÎncă nu există evaluări
- Employees' State Insurance Corporation E-Pehchan Card: Personal DetailsDocument2 paginiEmployees' State Insurance Corporation E-Pehchan Card: Personal DetailsPrashant KarekarÎncă nu există evaluări
- Employees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationDocument3 paginiEmployees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationRakesh Kumar MohantyÎncă nu există evaluări
- Employees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationDocument3 paginiEmployees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationRakesh Kumar MohantyÎncă nu există evaluări
- Employees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationDocument3 paginiEmployees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationRakesh Kumar MohantyÎncă nu există evaluări
- Employees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationDocument3 paginiEmployees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationRakesh Kumar MohantyÎncă nu există evaluări
- Employees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationDocument3 paginiEmployees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationRakesh Kumar MohantyÎncă nu există evaluări
- 0 - Scan Jun 27, 2019 PDFDocument2 pagini0 - Scan Jun 27, 2019 PDFAkshaya BalanÎncă nu există evaluări
- Employees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationDocument3 paginiEmployees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationRakesh Kumar MohantyÎncă nu există evaluări
- APHC Services 2022 ApplicationDocument2 paginiAPHC Services 2022 ApplicationKIRAN BABUÎncă nu există evaluări
- ApplicationDocument2 paginiApplicationhimanit405Încă nu există evaluări
- Employees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationDocument3 paginiEmployees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationRakesh Kumar MohantyÎncă nu există evaluări
- Employees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationDocument3 paginiEmployees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationRakesh Kumar MohantyÎncă nu există evaluări
- Employees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationDocument3 paginiEmployees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationRakesh Kumar MohantyÎncă nu există evaluări
- Employees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationDocument3 paginiEmployees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationRakesh Kumar MohantyÎncă nu există evaluări
- Abhishek Kumar ChoudharyDocument2 paginiAbhishek Kumar ChoudharyFor UseÎncă nu există evaluări
- Neet PG 2023Document4 paginiNeet PG 2023Chakra Teja ReddyÎncă nu există evaluări
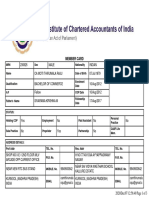
- Member CardDocument3 paginiMember CardthirumalarajuÎncă nu există evaluări
- Employees' State Insurance Corporation E-Pehchan Card: Personal DetailsDocument2 paginiEmployees' State Insurance Corporation E-Pehchan Card: Personal DetailsPravin PargiÎncă nu există evaluări
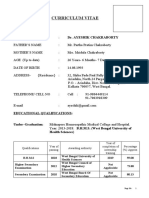
- Curriculum Vitae: Dr. Ayeshik ChakrabortyDocument3 paginiCurriculum Vitae: Dr. Ayeshik ChakrabortyAyeshik ChakrabortyÎncă nu există evaluări
- Employees' State Insurance Corporation E-Pehchan Card: Personal DetailsDocument2 paginiEmployees' State Insurance Corporation E-Pehchan Card: Personal DetailsAnil SharmaÎncă nu există evaluări
- Employees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationDocument3 paginiEmployees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationRakesh Kumar MohantyÎncă nu există evaluări
- About BlankDocument1 paginăAbout BlankPHOOL SINGH YADAVÎncă nu există evaluări
- Adobe Scan 28 Dec 2022Document7 paginiAdobe Scan 28 Dec 2022Prerana kaleÎncă nu există evaluări
- Abhishek EsicDocument2 paginiAbhishek Esicaschawda1414Încă nu există evaluări
- AdmitCard19745489 PDFDocument3 paginiAdmitCard19745489 PDFBeeru Singh baghelÎncă nu există evaluări
- Sparsh COMDocument2 paginiSparsh COMAvinash BaldiÎncă nu există evaluări
- M SrinivasDocument2 paginiM SrinivasPrince Kumar AzadÎncă nu există evaluări
- M Sandeep KumarDocument2 paginiM Sandeep KumarPrince Kumar AzadÎncă nu există evaluări
- Employees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationDocument3 paginiEmployees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationMythri Metallizing Pvt Ltd ProjectsÎncă nu există evaluări
- Employees' State Insurance Corporation E-Pehchan CardDocument2 paginiEmployees' State Insurance Corporation E-Pehchan Cardrupasana157Încă nu există evaluări
- Sujit Kumar Mahanta EsiDocument2 paginiSujit Kumar Mahanta Esisubhransusarangi0Încă nu există evaluări
- Employees' State Insurance Corporation E-Pehchan Card: Personal DetailsDocument2 paginiEmployees' State Insurance Corporation E-Pehchan Card: Personal DetailsPravin PargiÎncă nu există evaluări
- Employees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationDocument3 paginiEmployees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationRakesh Kumar MohantyÎncă nu există evaluări
- File 1 PDFDocument1 paginăFile 1 PDFMangal Singh RajawatÎncă nu există evaluări
- Recruitment Portal GACLDocument4 paginiRecruitment Portal GACLKhan FaizanÎncă nu există evaluări
- 3719060228Document2 pagini3719060228NISHANT395Încă nu există evaluări
- Registration Slip 2302640288Document2 paginiRegistration Slip 2302640288amansuriyanshi.gacÎncă nu există evaluări
- Application No. 2001 0001 577: Odisha Joint Entrance Examination - 2020 For B. Pharmacy/ INTEGRATED MBA (5YEARS)Document1 paginăApplication No. 2001 0001 577: Odisha Joint Entrance Examination - 2020 For B. Pharmacy/ INTEGRATED MBA (5YEARS)Anirudha ChoudhuryÎncă nu există evaluări
- List of Share Holders 2022Document1 paginăList of Share Holders 2022rahul.tibrewalÎncă nu există evaluări
- Employees' State Insurance Corporation E-Pehchan Card: Personal DetailsDocument2 paginiEmployees' State Insurance Corporation E-Pehchan Card: Personal DetailsvinodiipmÎncă nu există evaluări
- VasthuDocument1 paginăVasthuRam ReddyÎncă nu există evaluări
- All India Council For Technical Education: INSTITUTION DETAILS (Information Uploaded by Institute For Approval 2020-21)Document12 paginiAll India Council For Technical Education: INSTITUTION DETAILS (Information Uploaded by Institute For Approval 2020-21)Kishore JohnÎncă nu există evaluări
- Employees' State Insurance Corporation E-Pehchan Card: Personal DetailsDocument2 paginiEmployees' State Insurance Corporation E-Pehchan Card: Personal DetailsPravin PargiÎncă nu există evaluări
- Employees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationDocument3 paginiEmployees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationSSEworks GyÎncă nu există evaluări
- Interview Application Form-2023Document4 paginiInterview Application Form-2023Smc PowerÎncă nu există evaluări
- PREPGERN2100741 Gaurav AryaDocument3 paginiPREPGERN2100741 Gaurav AryaVineet KumarÎncă nu există evaluări
- 153/154, 4Th CRS, Dollars Clny, Opp. Clarence Public School, J P Nagar 4Th Phase, Bangalore, Karnataka-560078 Phone - 080-40402020Document1 pagină153/154, 4Th CRS, Dollars Clny, Opp. Clarence Public School, J P Nagar 4Th Phase, Bangalore, Karnataka-560078 Phone - 080-40402020pradeepshukla04Încă nu există evaluări
- Gecj 2021-22-4-67Document64 paginiGecj 2021-22-4-67GECJÎncă nu există evaluări
- Wipro Esic HemrajDocument2 paginiWipro Esic Hemrajbhartigiri26Încă nu există evaluări
- Application Form HCLFC409458Document3 paginiApplication Form HCLFC409458Rakesh KumarÎncă nu există evaluări
- DTE Naya Raipur ChhattisgarhDocument3 paginiDTE Naya Raipur Chhattisgarhsubham patraÎncă nu există evaluări
- Utkal University: This Form Should Not Be Submitted To Utkal UniversityDocument2 paginiUtkal University: This Form Should Not Be Submitted To Utkal UniversityKANHU SWAINÎncă nu există evaluări
- Employees' State Insurance Corporation E-Pehchan Card: Personal DetailsDocument2 paginiEmployees' State Insurance Corporation E-Pehchan Card: Personal DetailsPA PROJECTS PVT LTDÎncă nu există evaluări
- Employees' State Insurance Corporation E-Pehchan Card: Personal DetailsDocument2 paginiEmployees' State Insurance Corporation E-Pehchan Card: Personal Detailskunal monadlÎncă nu există evaluări
- Medical Reabursement GONo.74Document19 paginiMedical Reabursement GONo.74gsreddy100% (1)
- Appsc Dept - Test Eo 141 Test ResultsDocument35 paginiAppsc Dept - Test Eo 141 Test Resultsnavn7667% (3)
- Income Tax 2010-11 Version 11Document9 paginiIncome Tax 2010-11 Version 11gsreddyÎncă nu există evaluări
- Departmental Test Results GO TEST - CODE-88-97-May 2010Document28 paginiDepartmental Test Results GO TEST - CODE-88-97-May 2010Ramachandra RaoÎncă nu există evaluări
- Income Tax 2010-11 NewDocument11 paginiIncome Tax 2010-11 NewgsreddyÎncă nu există evaluări
- DA Software PRC 2010Document2 paginiDA Software PRC 2010gsreddyÎncă nu există evaluări
- Recognized Ho So ListDocument24 paginiRecognized Ho So ListJaganmohan BhatrajuÎncă nu există evaluări
- Income Tax 2010-11 Version 6Document4 paginiIncome Tax 2010-11 Version 6gsreddyÎncă nu există evaluări
- Income Tax 2010-11 (Version 1)Document4 paginiIncome Tax 2010-11 (Version 1)gsreddyÎncă nu există evaluări
- Income Tax 2010-11Document7 paginiIncome Tax 2010-11gsreddyÎncă nu există evaluări
- Income Tax 2010-11 Version 4Document4 paginiIncome Tax 2010-11 Version 4gsreddyÎncă nu există evaluări
- Income Tax 2010-11Document5 paginiIncome Tax 2010-11gsreddyÎncă nu există evaluări
- Income Tax 2010-11 Version 2Document4 paginiIncome Tax 2010-11 Version 2gsreddyÎncă nu există evaluări
- Income Tax 2010-11Document7 paginiIncome Tax 2010-11gsreddyÎncă nu există evaluări
- Remuneration For CodingDocument2 paginiRemuneration For CodinggsreddyÎncă nu există evaluări
- Income Tax 2010-11Document7 paginiIncome Tax 2010-11gsreddyÎncă nu există evaluări
- Don'T Delete This Sheet: (Mention Sri./Smt. Before Incumbent Name)Document22 paginiDon'T Delete This Sheet: (Mention Sri./Smt. Before Incumbent Name)gsreddyÎncă nu există evaluări
- DATA ENTRY SHEET (Enter Your Details) : (Mention Sri./Smt. Before Incumbent Name)Document22 paginiDATA ENTRY SHEET (Enter Your Details) : (Mention Sri./Smt. Before Incumbent Name)gsreddyÎncă nu există evaluări
- Basic InvoiceDocument1 paginăBasic InvoicegsreddyÎncă nu există evaluări
- Promotions ScheduleDocument1 paginăPromotions SchedulegsreddyÎncă nu există evaluări
- ZPPF Closer ApplicationDocument6 paginiZPPF Closer ApplicationgsreddyÎncă nu există evaluări
- PRC 2010 Fixation Principles RulesDocument17 paginiPRC 2010 Fixation Principles RulesSEKHAR100% (3)
- Remuneration For Exam DutiesDocument2 paginiRemuneration For Exam DutiesgsreddyÎncă nu există evaluări
- ZPPF Number Allottment ApplicationDocument5 paginiZPPF Number Allottment ApplicationgsreddyÎncă nu există evaluări
- CCCCDocument91 paginiCCCCgsreddyÎncă nu există evaluări
- Instructions To Use This ProgrammeDocument192 paginiInstructions To Use This ProgrammegsreddyÎncă nu există evaluări
- ZPPF Loan Recoverable ApplicationDocument3 paginiZPPF Loan Recoverable ApplicationNaga ManoharababuÎncă nu există evaluări
- DSE ProcdgsDocument1 paginăDSE ProcdgsgsreddyÎncă nu există evaluări
- National Programme of Mid-Day Meal in Schools PAB Approved Number of School Working Days (Primary & Upper Primary Classes I-VIII) For 2010-11Document31 paginiNational Programme of Mid-Day Meal in Schools PAB Approved Number of School Working Days (Primary & Upper Primary Classes I-VIII) For 2010-11gsreddyÎncă nu există evaluări
- BCPC ResoDocument2 paginiBCPC Resopao lonzagaÎncă nu există evaluări
- ITAT Holds That Charitable Trust Running Max Hospital Was Charitable To Only To Corporate Max Group of Companies and Uncharitable' Towards The Society or PublicDocument46 paginiITAT Holds That Charitable Trust Running Max Hospital Was Charitable To Only To Corporate Max Group of Companies and Uncharitable' Towards The Society or PublicLive LawÎncă nu există evaluări
- RHMP Registration-FormDocument3 paginiRHMP Registration-FormKaleem HashmiÎncă nu există evaluări
- Draft Resolution No. 58-2020 - Authorizing Mayor To Sign Deed of Donation With PCSO For Patient Transport VehicleDocument2 paginiDraft Resolution No. 58-2020 - Authorizing Mayor To Sign Deed of Donation With PCSO For Patient Transport VehicleRica Carmel Lanzaderas100% (2)
- 47.HDEC-HSE-F0047 Pressure Test PermitDocument1 pagină47.HDEC-HSE-F0047 Pressure Test PermitRonn CaiÎncă nu există evaluări
- Diana M Cabarcas UparelaDocument8 paginiDiana M Cabarcas UparelaDianaÎncă nu există evaluări
- Relig AreDocument5 paginiRelig AresomnathÎncă nu există evaluări
- Colorado House Bill 13-1114Document20 paginiColorado House Bill 13-1114Medicinal ColoradoÎncă nu există evaluări
- Fire SafetyDocument19 paginiFire SafetyZulvita AmandaÎncă nu există evaluări
- The Tools of Government A Guide To The New Governance 1st EditionDocument61 paginiThe Tools of Government A Guide To The New Governance 1st Editionwillie.getz795100% (39)
- Pre Joining GuidelinesDocument21 paginiPre Joining GuidelinesHarsha VardhanÎncă nu există evaluări
- NZ USAR Capabiity in 2001Document20 paginiNZ USAR Capabiity in 2001Shane BriggsÎncă nu există evaluări
- Mate Rio VigilanceDocument4 paginiMate Rio VigilanceilyasÎncă nu există evaluări
- Candace Steel LawsuitDocument20 paginiCandace Steel LawsuitMichelleÎncă nu există evaluări
- 2016 Xyngular Income Summary 100316.01v3Document1 pagină2016 Xyngular Income Summary 100316.01v3Asish BeheraÎncă nu există evaluări
- State ContactsDocument581 paginiState ContactsSunil Pandey100% (1)
- Fact Sheet Health InsuranceDocument4 paginiFact Sheet Health Insuranceph.lawÎncă nu există evaluări
- For The Latest Information On Labor Education Assistance Program (LEAP), Visit The IATSE's Web Site atDocument40 paginiFor The Latest Information On Labor Education Assistance Program (LEAP), Visit The IATSE's Web Site atIATSEÎncă nu există evaluări
- Combined Lobbyist List by Registrant With Type of Lobbying and IssuesDocument1.101 paginiCombined Lobbyist List by Registrant With Type of Lobbying and IssuesJordan FensterÎncă nu există evaluări
- Mobile ConnectionsDocument24 paginiMobile Connectionsarchana bhanushaliÎncă nu există evaluări
- Speech by RT Hon Prime Minister On Sickle Cell AnaemiaDocument4 paginiSpeech by RT Hon Prime Minister On Sickle Cell AnaemiaEdwin Kemboi100% (1)
- March 2013 NewsletterDocument2 paginiMarch 2013 Newsletterapi-79187448Încă nu există evaluări
- Lubrication Identification Tag Best Practices and InnovationsDocument3 paginiLubrication Identification Tag Best Practices and InnovationsManuel LombarderoÎncă nu există evaluări
- CBRO Drug Control Dept.Document7 paginiCBRO Drug Control Dept.Anil KumarÎncă nu există evaluări
- UU Keselamatan Kerja English VersionDocument15 paginiUU Keselamatan Kerja English VersionPurwani HandayaniÎncă nu există evaluări
- Prospectus AIPGDEE 2015Document65 paginiProspectus AIPGDEE 2015Neepur GargÎncă nu există evaluări
- Petition of Private Criminal Complaint in Lancaster County Court of Common Pleas Clerk of Court v. Lancaster City Police For 302 Warrant of July 9, 2015 Filed September 23, 2015Document123 paginiPetition of Private Criminal Complaint in Lancaster County Court of Common Pleas Clerk of Court v. Lancaster City Police For 302 Warrant of July 9, 2015 Filed September 23, 2015Stan J. CaterboneÎncă nu există evaluări
- Structure of Urban Local Government - KarnatakaDocument25 paginiStructure of Urban Local Government - KarnatakaChhabi YadavÎncă nu există evaluări
- Barangay Nutrition Council: Republic of The Philippines Province of Catanduanes Municipality of Virac Barangay San PabloDocument6 paginiBarangay Nutrition Council: Republic of The Philippines Province of Catanduanes Municipality of Virac Barangay San Pablojinky guerrero80% (5)
- Bhopal Disaster: From Wikipedia, The Free EncyclopediaDocument17 paginiBhopal Disaster: From Wikipedia, The Free Encyclopediamanoj_mafiosiÎncă nu există evaluări