S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- LSD OD Westjmed00307-0025 PDFDocument6 paginiLSD OD Westjmed00307-0025 PDF0j1u9nmkv534vw9vÎncă nu există evaluări
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
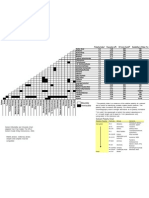
- Solvent Miscibility and Polarity ChartDocument1 paginăSolvent Miscibility and Polarity Chartdiptafara100% (3)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Coma, Hyperthermia and Bleeding Associated With Massive LSD OverdoseDocument6 paginiComa, Hyperthermia and Bleeding Associated With Massive LSD Overdose0j1u9nmkv534vw9vÎncă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- King Scientific CatalogueDocument694 paginiKing Scientific Catalogue0j1u9nmkv534vw9v100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Pressure Conversion TableDocument1 paginăPressure Conversion Table0j1u9nmkv534vw9vÎncă nu există evaluări
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Synthesis of Amides of Lysergic AcidDocument5 paginiSynthesis of Amides of Lysergic Acid0j1u9nmkv534vw9v100% (1)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- LSD and Its Lysergamide CousinsDocument8 paginiLSD and Its Lysergamide Cousins0j1u9nmkv534vw9vÎncă nu există evaluări
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Characterization of 2 - (3-Methoxyphenyl) - 2 - (Ethylamino) Cyclohexanone (Methoxetamine)Document15 paginiThe Characterization of 2 - (3-Methoxyphenyl) - 2 - (Ethylamino) Cyclohexanone (Methoxetamine)0j1u9nmkv534vw9vÎncă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- UK Government Drug Precursors Wallchart Update February 2012Document2 paginiUK Government Drug Precursors Wallchart Update February 20120j1u9nmkv534vw9vÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Adobe Scan 24 May 2023Document1 paginăAdobe Scan 24 May 2023nemoÎncă nu există evaluări
- Goodwill Magazine For WebsiteDocument23 paginiGoodwill Magazine For WebsiteMARK ANTHONY ALCANTARAÎncă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- 5.4-8 Good HousekeepingDocument4 pagini5.4-8 Good HousekeepingMylina FabiÎncă nu există evaluări
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- MD3 Peer TutoringDocument3 paginiMD3 Peer Tutoringdragtoss2Încă nu există evaluări
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Obat THTDocument3 paginiObat THTSartikaOdockÎncă nu există evaluări
- Applied Sociology 2.0Document14 paginiApplied Sociology 2.0Roy Alcoriza AriosaÎncă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Hourglass Sculpt: With Lilly SabriDocument6 paginiHourglass Sculpt: With Lilly SabriRukhsana ShahÎncă nu există evaluări
- Nutrimax FebruariDocument24 paginiNutrimax Februarikimiafarma 79Încă nu există evaluări
- Imported Medical Devices - Class - ADocument32 paginiImported Medical Devices - Class - AMd. Shafi NewazÎncă nu există evaluări
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Recreation and Other Social Welfare Concerns: Lesson 27Document30 paginiRecreation and Other Social Welfare Concerns: Lesson 27Rachelle PitpitÎncă nu există evaluări
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Biochemical Mechanism of Vitamin A in VisionDocument3 paginiBiochemical Mechanism of Vitamin A in VisionAurelia HernandezÎncă nu există evaluări
- Joint Press Release 042820Document2 paginiJoint Press Release 042820Alyssa EstesÎncă nu există evaluări
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- ODSP APPLICATION FORM (Incoming 1st Year and Continuing Students)Document4 paginiODSP APPLICATION FORM (Incoming 1st Year and Continuing Students)Ha50% (4)
- Gaslighting Research EssayDocument9 paginiGaslighting Research Essayapi-519870004Încă nu există evaluări
- Breast Cancer Cell LineDocument34 paginiBreast Cancer Cell LineCatherine RajanÎncă nu există evaluări
- Many Social Organisation and Women Activist Took Up Bhanwari DeviDocument91 paginiMany Social Organisation and Women Activist Took Up Bhanwari DeviRubal Tajender MalikÎncă nu există evaluări
- Standard of Duty of Care-03Document34 paginiStandard of Duty of Care-03burnercum69Încă nu există evaluări
- Absenteeism in The Workplace 1Document8 paginiAbsenteeism in The Workplace 1Raihannisa AzizahÎncă nu există evaluări
- Personality and Individual Di FferencesDocument7 paginiPersonality and Individual Di FferencesDarojaturroofi'ah SodiqÎncă nu există evaluări
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Health Education Reviewer (Midterm)Document6 paginiHealth Education Reviewer (Midterm)Carrie Anne Aquila GarciaÎncă nu există evaluări
- FDA 483 and Warning LetterDocument38 paginiFDA 483 and Warning LetterOmar FaruqÎncă nu există evaluări
- The History of Neurosurgery in Bolivia and PediatrDocument7 paginiThe History of Neurosurgery in Bolivia and PediatrMarcela Sanchez ParraÎncă nu există evaluări
- Behavior Analysis in Education Final.22Document12 paginiBehavior Analysis in Education Final.22Bea Dimaun100% (1)
- Critique PaperDocument2 paginiCritique PaperDaisy Mae GujolÎncă nu există evaluări
- GE Panda Ires Warmer Operation and Maintenance ManualDocument90 paginiGE Panda Ires Warmer Operation and Maintenance Manualiman hilmanÎncă nu există evaluări
- Psy 222 Sim - Week 1 - 9Document241 paginiPsy 222 Sim - Week 1 - 9Angel Delos Santos AtosÎncă nu există evaluări
- The Importance of Employee Engagement in Mediating The Improvement of Staff Performance at The HospitalDocument12 paginiThe Importance of Employee Engagement in Mediating The Improvement of Staff Performance at The HospitalNadia ShabrinaÎncă nu există evaluări
- Resume For PortfolioDocument2 paginiResume For Portfolioapi-546575413Încă nu există evaluări
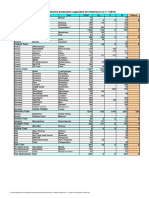
- Installed Chlorine Production Capacities (KT Chlorine/yr On 1-1-2016)Document2 paginiInstalled Chlorine Production Capacities (KT Chlorine/yr On 1-1-2016)keo landÎncă nu există evaluări
- Drug StudyDocument4 paginiDrug StudyPam RomeroÎncă nu există evaluări
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)