S-ar putea să vă placă și
- Orthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentDe la EverandOrthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentFederico BrugnamiÎncă nu există evaluări
- Implant and Periodontal ConsiderationsDocument53 paginiImplant and Periodontal ConsiderationsAlphonse ThangapradeepÎncă nu există evaluări
- Emerging Nanotechnologies in DentistryDe la EverandEmerging Nanotechnologies in DentistryKarthikeyan SubramaniÎncă nu există evaluări
- A New Classification Scheme For Periodontal and Peri-Implant Diseases and Conditions - Introduction and Key Changes From The 1999 ClassificationDocument8 paginiA New Classification Scheme For Periodontal and Peri-Implant Diseases and Conditions - Introduction and Key Changes From The 1999 Classificationvaleria Gonzalez BalloteÎncă nu există evaluări
- Berglundh Et Al (2018) - Peri Implant Diseases and Conditions - Consensus Report of Workgroup 4 - 1Document9 paginiBerglundh Et Al (2018) - Peri Implant Diseases and Conditions - Consensus Report of Workgroup 4 - 1FelipeOyarceSalazarÎncă nu există evaluări
- Peri Implant Disease PDFDocument32 paginiPeri Implant Disease PDFHajra FarooqÎncă nu există evaluări
- Endodontics or Implants. A Review of Decisive Criteria and GuidelinesDocument19 paginiEndodontics or Implants. A Review of Decisive Criteria and GuidelinesJuan David Torres CanoÎncă nu există evaluări
- Peri Implantitisetiologydiagnosisandmanagement PDFDocument49 paginiPeri Implantitisetiologydiagnosisandmanagement PDFRobins DhakalÎncă nu există evaluări
- 5 PDFDocument8 pagini5 PDFoskar ORTIZÎncă nu există evaluări
- Gingival Retraction Techniques: A Review: Dental Update April 2018Document10 paginiGingival Retraction Techniques: A Review: Dental Update April 2018Varun bharathiÎncă nu există evaluări
- Medical Engineering & PhysicsDocument6 paginiMedical Engineering & PhysicsLuis Fernando Guayllas PomaÎncă nu există evaluări
- #1 Rationale ImplantDocument5 pagini#1 Rationale Implantsohaib197Încă nu există evaluări
- Journal ClubDocument15 paginiJournal Clubperiodontics07Încă nu există evaluări
- Laser in PerioDocument24 paginiLaser in Periodhwanit31Încă nu există evaluări
- Transitioning Patients From Teeth To ImplantsDocument11 paginiTransitioning Patients From Teeth To ImplantsAlexandra DumitracheÎncă nu există evaluări
- 2006 Implant SurfacesDocument16 pagini2006 Implant SurfacesLukas Lopez RamirezÎncă nu există evaluări
- Berglundh Et Al-2018-Journal of Clinical PeriodontologyDocument6 paginiBerglundh Et Al-2018-Journal of Clinical PeriodontologyCristian CulcitchiÎncă nu există evaluări
- Perio 2000 VOL-76 Treatment of Pathologic Peri-Implant Pocket PDFDocument11 paginiPerio 2000 VOL-76 Treatment of Pathologic Peri-Implant Pocket PDFchandanaÎncă nu există evaluări
- Implant Loading Protocols For The Partially Edentulous Esthetic ZoneDocument11 paginiImplant Loading Protocols For The Partially Edentulous Esthetic ZoneKarla AlanisÎncă nu există evaluări
- Peri-Implantitis: Presented By: Kriti Dalmia. Moderated By: Dr. Shobha RDocument29 paginiPeri-Implantitis: Presented By: Kriti Dalmia. Moderated By: Dr. Shobha RDr Farhat100% (1)
- UntitledDocument70 paginiUntitledPerebyinis PavloÎncă nu există evaluări
- Prevention of Peri Implantitis A Narrative Review1Document7 paginiPrevention of Peri Implantitis A Narrative Review1asdÎncă nu există evaluări
- Dental Implants: Dr. D.M. Ajayi. August, 2017Document129 paginiDental Implants: Dr. D.M. Ajayi. August, 2017Kassim OboghenaÎncă nu există evaluări
- Oral Diagnosis and Treatment Planning: Part 7. Treatment Planning For Missing TeethDocument11 paginiOral Diagnosis and Treatment Planning: Part 7. Treatment Planning For Missing TeethalfredoibcÎncă nu există evaluări
- Implant Maintenance - A Clinical UpdateDocument9 paginiImplant Maintenance - A Clinical UpdateDr. Minkle GulatiÎncă nu există evaluări
- The Effect of Implant Abutment Junction Position On Crestal Bone Loss A Systematic Review and Meta AnalysisDocument17 paginiThe Effect of Implant Abutment Junction Position On Crestal Bone Loss A Systematic Review and Meta AnalysisBagis Emre GulÎncă nu există evaluări
- Immediate Loading Principles - Requirements - and Soft-Tissue Management PDFDocument11 paginiImmediate Loading Principles - Requirements - and Soft-Tissue Management PDFMahmoud Ahmad100% (1)
- Classification of Facial Peri-Implant Soft Tissue Zucchelli 2019 ColDocument9 paginiClassification of Facial Peri-Implant Soft Tissue Zucchelli 2019 ColSebastián BernalÎncă nu există evaluări
- Preprosthetic and Reconstructive SurgeryDocument32 paginiPreprosthetic and Reconstructive Surgeryruoiconmapu100% (1)
- Generic Root Form Component Terminology: Carl E. MischDocument11 paginiGeneric Root Form Component Terminology: Carl E. MischbubuvulpeaÎncă nu există evaluări
- Rethinking FerruleDocument10 paginiRethinking FerruleteodudeÎncă nu există evaluări
- 0 - A Clinical Guide To OcclusionDocument1 pagină0 - A Clinical Guide To Occlusionyhajo100% (1)
- The Role and Various Uses of Laser in Oral and Maxillofacial SurgeryDocument54 paginiThe Role and Various Uses of Laser in Oral and Maxillofacial SurgeryObinna IgwiloÎncă nu există evaluări
- Implant Occlusion Articles AbstractDocument4 paginiImplant Occlusion Articles AbstractMrunal DoiphodeÎncă nu există evaluări
- Relationship Between Bruxism and Temporomandibular Disorders: A Systematic Review of Literature From 1998 To 2008Document25 paginiRelationship Between Bruxism and Temporomandibular Disorders: A Systematic Review of Literature From 1998 To 2008AARON DIAZ RONQUILLOÎncă nu există evaluări
- The Biophysics of Mandibular Fractures - An Evolution Toward UnderstandingDocument13 paginiThe Biophysics of Mandibular Fractures - An Evolution Toward UnderstandingMikeunoeÎncă nu există evaluări
- JC 11 A Systematic Review of The Survival and ComplicationDocument41 paginiJC 11 A Systematic Review of The Survival and ComplicationMrinmayee ThakurÎncă nu există evaluări
- Os SEO IntegrationDocument45 paginiOs SEO IntegrationDrKrishna DasÎncă nu există evaluări
- Implant Course.Document76 paginiImplant Course.mustafaÎncă nu există evaluări
- Oral ImplantologyDocument26 paginiOral ImplantologyPrathik RaiÎncă nu există evaluări
- Peri-Implantitis: A Curse To ImplantsDocument11 paginiPeri-Implantitis: A Curse To ImplantsIJRASETPublicationsÎncă nu există evaluări
- Crestal Bone Changes On Platform - Switched Implants and Adjacent Teeth When The Tooth-Implant Distance Is Less Than 1.5 MMDocument10 paginiCrestal Bone Changes On Platform - Switched Implants and Adjacent Teeth When The Tooth-Implant Distance Is Less Than 1.5 MMJuanOso Gutierrez ArayaÎncă nu există evaluări
- Renvert Et Al (2018) - Peri Implant Health, Peri Implant Mucositis, and Peri Implantitis - Case Definitions and Diagnostic Considerations - 1Document9 paginiRenvert Et Al (2018) - Peri Implant Health, Peri Implant Mucositis, and Peri Implantitis - Case Definitions and Diagnostic Considerations - 1FelipeOyarceSalazarÎncă nu există evaluări
- Schwarz Et Al (2018) - Peri Implantitis - 1Document23 paginiSchwarz Et Al (2018) - Peri Implantitis - 1FelipeOyarceSalazarÎncă nu există evaluări
- 2010 - Rossouw, PE - A Historical Overview of The Development of The Acid Etch Bonding System in OrthodonticsDocument22 pagini2010 - Rossouw, PE - A Historical Overview of The Development of The Acid Etch Bonding System in Orthodonticsbajobajic100% (1)
- Implant Failure and Their ManagementDocument61 paginiImplant Failure and Their ManagementDharshiniÎncă nu există evaluări
- Peri-Implantitis: Srijana Heka Bds Iv Year Roll No: 17Document60 paginiPeri-Implantitis: Srijana Heka Bds Iv Year Roll No: 17cz22naÎncă nu există evaluări
- 3.factors and Techniques Influencing Peri-Implant Papillae - PDFDocument12 pagini3.factors and Techniques Influencing Peri-Implant Papillae - PDFMargarita María Blanco LópezÎncă nu există evaluări
- Digital Impression 2022Document23 paginiDigital Impression 2022AseelÎncă nu există evaluări
- Ke Principles of Implant Dentistr in The Esthetic Zone: Michael Sonick, DMD Debb Hwang, DMDDocument6 paginiKe Principles of Implant Dentistr in The Esthetic Zone: Michael Sonick, DMD Debb Hwang, DMDVikas Aggarwal100% (1)
- Post-Surgical Complications and Management in Dental ImplantsDocument41 paginiPost-Surgical Complications and Management in Dental ImplantspipyirÎncă nu există evaluări
- Osseointegration of Bone ImplantsDocument15 paginiOsseointegration of Bone ImplantsBaris BogazkesenliÎncă nu există evaluări
- Peri-Implant Health, Peri-Implant Mucositis, and Peri-Implantitis: Case Definitions and Diagnostic ConsiderationsDocument9 paginiPeri-Implant Health, Peri-Implant Mucositis, and Peri-Implantitis: Case Definitions and Diagnostic ConsiderationsFrancisca Cardenas OñateÎncă nu există evaluări
- Whale's Tail TechniqueDocument32 paginiWhale's Tail Techniquevijeta vyasÎncă nu există evaluări
- Biological Properties of Dental Materials 1-General Dentistry / Orthodontic Courses by Indian Dental AcademyDocument76 paginiBiological Properties of Dental Materials 1-General Dentistry / Orthodontic Courses by Indian Dental Academyindian dental academyÎncă nu există evaluări
- Chapter 6 Midi Implant ProcedureDocument9 paginiChapter 6 Midi Implant Procedurezeus_1949Încă nu există evaluări
- Management of Peri-Implant Mucositis and Peri-Implantitis PDFDocument19 paginiManagement of Peri-Implant Mucositis and Peri-Implantitis PDFgirl33Încă nu există evaluări
- Nanohybrid Versus Nano LL Composite in Class I CavitiesDocument5 paginiNanohybrid Versus Nano LL Composite in Class I CavitiessonygabrielÎncă nu există evaluări
- Published Immediate ImplantDocument6 paginiPublished Immediate Implantshayma rafatÎncă nu există evaluări
- Complete Denture TechniquesDocument6 paginiComplete Denture TechniquesJohn Hyunuk ChoÎncă nu există evaluări
- Oral Maxillofac Surg Clin North Am v.b20, n.b02, May 2008Document164 paginiOral Maxillofac Surg Clin North Am v.b20, n.b02, May 2008Ledir Luciana Henley de AndradeÎncă nu există evaluări
- Severe Anterior Open Bite With Mandibular Retrusion Treated With Multiloop Edgewise Archwires and Microimplant Anchorage ComplementedDocument10 paginiSevere Anterior Open Bite With Mandibular Retrusion Treated With Multiloop Edgewise Archwires and Microimplant Anchorage ComplementedLedir Luciana Henley de AndradeÎncă nu există evaluări
- The Positioning and Magnification of Faces and Skulls For Photographic SuperimpositionDocument11 paginiThe Positioning and Magnification of Faces and Skulls For Photographic SuperimpositionLedir Luciana Henley de AndradeÎncă nu există evaluări
- Horizontal and Vertical Ridge Augmentation in Localized Alveolar Deficient Sites - A Retrospective Case Series PDFDocument11 paginiHorizontal and Vertical Ridge Augmentation in Localized Alveolar Deficient Sites - A Retrospective Case Series PDFLedir Luciana Henley de AndradeÎncă nu există evaluări
- A Longitudinal Study of Combined Periodontal and Prosthetic Treatment of Patients With Advanced Periodontal DiseaseDocument7 paginiA Longitudinal Study of Combined Periodontal and Prosthetic Treatment of Patients With Advanced Periodontal DiseaseLedir Luciana Henley de AndradeÎncă nu există evaluări
- Association of Lip Pigmentation With Smoking and Gingival Melanin PigmentationDocument6 paginiAssociation of Lip Pigmentation With Smoking and Gingival Melanin PigmentationLedir Luciana Henley de AndradeÎncă nu există evaluări
- A Cephalometric Evaluation of The Dental and Facial-Skeletal Effects Using The Bionator With Stepwise Protrusive ActivationsDocument8 paginiA Cephalometric Evaluation of The Dental and Facial-Skeletal Effects Using The Bionator With Stepwise Protrusive ActivationsLedir Luciana Henley de AndradeÎncă nu există evaluări
- Using Orthodontic Intrusion of Abraded Incisors To Facilitate Restoration The Technique's Effects On Alveolar Bone Level and Root LengthDocument10 paginiUsing Orthodontic Intrusion of Abraded Incisors To Facilitate Restoration The Technique's Effects On Alveolar Bone Level and Root LengthLedir Luciana Henley de AndradeÎncă nu există evaluări
- A Case Series On Crestal Sinus Elevation With Rotary InstrumentsDocument8 paginiA Case Series On Crestal Sinus Elevation With Rotary InstrumentsLedir Luciana Henley de AndradeÎncă nu există evaluări
- Logy A Clinical Textbook 2009Document502 paginiLogy A Clinical Textbook 2009Ledir Luciana Henley de AndradeÎncă nu există evaluări
- Calcium Silicate Block and Pipe Thermal Insulation: Standard Specification ForDocument4 paginiCalcium Silicate Block and Pipe Thermal Insulation: Standard Specification ForNour MasmoudiÎncă nu există evaluări
- Cbse Class 9 Science Solved Practice Paper Set IDocument19 paginiCbse Class 9 Science Solved Practice Paper Set IDhiraj PadamwarÎncă nu există evaluări
- Studi Kasus Kandungan Formalin Pada Ikan Teri Nasi (Stolephorus Commersoni Lac.) Asin Kering Di Pasar Rau Serang Banten - DocDocument4 paginiStudi Kasus Kandungan Formalin Pada Ikan Teri Nasi (Stolephorus Commersoni Lac.) Asin Kering Di Pasar Rau Serang Banten - DocRini YanuartiÎncă nu există evaluări
- EOCQ Ans 6Document2 paginiEOCQ Ans 6harshanauoc100% (2)
- NF6.1FX.2 Standard Compressor R134a 115-127V 60Hz: GeneralDocument2 paginiNF6.1FX.2 Standard Compressor R134a 115-127V 60Hz: Generalwilmer cantilloÎncă nu există evaluări
- TmaDocument5 paginiTmaShan Dela VegaÎncă nu există evaluări
- Sika Viscocrete: TechnologyDocument13 paginiSika Viscocrete: TechnologyacarthurÎncă nu există evaluări
- NEET/JEE: 2020-21: Periodic PropertiesDocument3 paginiNEET/JEE: 2020-21: Periodic Propertiesshantinath123gmailcoÎncă nu există evaluări
- Hempel Protective Infrastructure Corrosion Protection For Cargo Handling Equipment Low ResDocument12 paginiHempel Protective Infrastructure Corrosion Protection For Cargo Handling Equipment Low Reskamardheen majithÎncă nu există evaluări
- PhysicsDocument396 paginiPhysicsGreeny34Încă nu există evaluări
- 87 Kerabondplus GB in PDFDocument4 pagini87 Kerabondplus GB in PDFpankajÎncă nu există evaluări
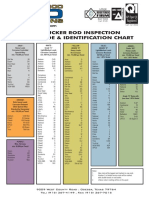
- Permian Rod Operations - Sucker Rod Identification Chart PDFDocument1 paginăPermian Rod Operations - Sucker Rod Identification Chart PDFMinimaxou78Încă nu există evaluări
- Alchemy at The Crowning of NatureDocument30 paginiAlchemy at The Crowning of NatureMano DasruthiÎncă nu există evaluări
- Requisitions IndexDocument13 paginiRequisitions IndexKarnan ThirugnanamÎncă nu există evaluări
- Spider SilkDocument5 paginiSpider SilkimranÎncă nu există evaluări
- CH 06Document18 paginiCH 06Abdul Shokor Abd TalibÎncă nu există evaluări
- Unidad 6 Orificios. Vertederos Y Resalto HidráulicoDocument5 paginiUnidad 6 Orificios. Vertederos Y Resalto HidráulicoPascual JhonnÎncă nu există evaluări
- Rydlyme: The Solution To Your Water Scale ProblemsDocument4 paginiRydlyme: The Solution To Your Water Scale Problemswq3erwqerwerÎncă nu există evaluări
- Design of Cold Storage Structure For Thousand PDFDocument8 paginiDesign of Cold Storage Structure For Thousand PDFzhyhhÎncă nu există evaluări
- Free Particle PropagatorDocument2 paginiFree Particle PropagatorstephenbankesÎncă nu există evaluări
- Resitivity LogDocument30 paginiResitivity LogMuhammad AneesÎncă nu există evaluări
- ABB Raw Mix Preparation PDFDocument8 paginiABB Raw Mix Preparation PDFrudye kardun100% (1)
- STAT152 Test Prep 1Document6 paginiSTAT152 Test Prep 1Hilmi HusinÎncă nu există evaluări
- mp1 2 PDFDocument1 paginămp1 2 PDFAmer MehmoodÎncă nu există evaluări
- Titration of Sodium Hydroxide With Hydrochloric AcidDocument3 paginiTitration of Sodium Hydroxide With Hydrochloric AcidMir HashemiÎncă nu există evaluări
- Phystcs B (Advancing Physics) U Nderstanding Processes: Friday AfternoonDocument21 paginiPhystcs B (Advancing Physics) U Nderstanding Processes: Friday AfternoonKelen KawasakiÎncă nu există evaluări
- Bulletin RHIDocument76 paginiBulletin RHIwaqasaziz786Încă nu există evaluări
- Is 13871 1993 Powder Coating SpecificationDocument14 paginiIs 13871 1993 Powder Coating SpecificationArunashish Mazumdar50% (2)
- Hysteretic Relative Permeability EffectsDocument8 paginiHysteretic Relative Permeability Effectshfdshy12Încă nu există evaluări
- ME Vol 2 FMDocument364 paginiME Vol 2 FMDeepak Gupta100% (4)
- Rocks and Minerals of The World: Geology for Kids - Minerology and SedimentologyDe la EverandRocks and Minerals of The World: Geology for Kids - Minerology and SedimentologyEvaluare: 4.5 din 5 stele4.5/5 (5)
- The Things We Make: The Unknown History of Invention from Cathedrals to Soda CansDe la EverandThe Things We Make: The Unknown History of Invention from Cathedrals to Soda CansEvaluare: 4.5 din 5 stele4.5/5 (21)
- The Things We Make: The Unknown History of Invention from Cathedrals to Soda Cans (Father's Day Gift for Science and Engineering Curious Dads)De la EverandThe Things We Make: The Unknown History of Invention from Cathedrals to Soda Cans (Father's Day Gift for Science and Engineering Curious Dads)Încă nu există evaluări
- Composite Structures of Steel and Concrete: Beams, Slabs, Columns and Frames for BuildingsDe la EverandComposite Structures of Steel and Concrete: Beams, Slabs, Columns and Frames for BuildingsÎncă nu există evaluări
- To Engineer Is Human: The Role of Failure in Successful DesignDe la EverandTo Engineer Is Human: The Role of Failure in Successful DesignEvaluare: 4 din 5 stele4/5 (138)
- The Great Bridge: The Epic Story of the Building of the Brooklyn BridgeDe la EverandThe Great Bridge: The Epic Story of the Building of the Brooklyn BridgeEvaluare: 4.5 din 5 stele4.5/5 (59)
- Skyway: The True Story of Tampa Bay's Signature Bridge and the Man Who Brought It DownDe la EverandSkyway: The True Story of Tampa Bay's Signature Bridge and the Man Who Brought It DownÎncă nu există evaluări
- Troubleshooting and Repair of Diesel EnginesDe la EverandTroubleshooting and Repair of Diesel EnginesEvaluare: 1.5 din 5 stele1.5/5 (2)
- Crossings: How Road Ecology Is Shaping the Future of Our PlanetDe la EverandCrossings: How Road Ecology Is Shaping the Future of Our PlanetEvaluare: 4.5 din 5 stele4.5/5 (10)
- Predicting Lifetime for Concrete StructureDe la EverandPredicting Lifetime for Concrete StructureÎncă nu există evaluări
- Structural Cross Sections: Analysis and DesignDe la EverandStructural Cross Sections: Analysis and DesignEvaluare: 4.5 din 5 stele4.5/5 (19)
- Geotechnical Engineering Calculations and Rules of ThumbDe la EverandGeotechnical Engineering Calculations and Rules of ThumbEvaluare: 4 din 5 stele4/5 (17)
- Summary of Mark Owens & Delia Owens's Cry Of The KalahariDe la EverandSummary of Mark Owens & Delia Owens's Cry Of The KalahariÎncă nu există evaluări
- Finite Element Analysis and Design of Steel and Steel–Concrete Composite BridgesDe la EverandFinite Element Analysis and Design of Steel and Steel–Concrete Composite BridgesÎncă nu există evaluări
- Structural Analysis 1: Statically Determinate StructuresDe la EverandStructural Analysis 1: Statically Determinate StructuresÎncă nu există evaluări
- Summary of Taiichi Ohno's Taiichi Ohno's Workplace ManagementDe la EverandSummary of Taiichi Ohno's Taiichi Ohno's Workplace ManagementÎncă nu există evaluări
- Rock Fracture and Blasting: Theory and ApplicationsDe la EverandRock Fracture and Blasting: Theory and ApplicationsEvaluare: 5 din 5 stele5/5 (2)
- CAREC Road Safety Engineering Manual 3: Roadside Hazard ManagementDe la EverandCAREC Road Safety Engineering Manual 3: Roadside Hazard ManagementÎncă nu există evaluări