S-ar putea să vă placă și
- Dimensional PsychopathologyDe la EverandDimensional PsychopathologyMassimo BiondiÎncă nu există evaluări
- Psychosocial Work Environment and Stress-Related Disorders, A Systematic ReviewDocument10 paginiPsychosocial Work Environment and Stress-Related Disorders, A Systematic ReviewBegoña MartinezÎncă nu există evaluări
- Psychosocial Work Environment and Stress-Related Disorders, A Systematic ReviewDocument10 paginiPsychosocial Work Environment and Stress-Related Disorders, A Systematic Reviewreza30 dilagaÎncă nu există evaluări
- Psychosocial Work Environment and Stress-Related Disorders, A Systematic ReviewDocument11 paginiPsychosocial Work Environment and Stress-Related Disorders, A Systematic ReviewPatriciaÎncă nu există evaluări
- A Systematic Review of Studies in The Contributions of The Work Environment To Ischaemic Heart Disease DevelopmentDocument8 paginiA Systematic Review of Studies in The Contributions of The Work Environment To Ischaemic Heart Disease DevelopmentKurnia Fitri AprillianaÎncă nu există evaluări
- KQW 161Document6 paginiKQW 161andres felipeÎncă nu există evaluări
- Workstyle Measure: Short Form: January 2005Document7 paginiWorkstyle Measure: Short Form: January 2005Diyandaru AdhityaÎncă nu există evaluări
- Dissecting The Effect of Workplace Exposures On Workers ' Rating of Psychological Health and SafetyDocument10 paginiDissecting The Effect of Workplace Exposures On Workers ' Rating of Psychological Health and SafetyEgle UselieneÎncă nu există evaluări
- PrevalenceofstressDocument13 paginiPrevalenceofstressTrương Bình TrọngÎncă nu există evaluări
- Occupational Stress in Physical Therapist Working As Clinician and Academician in Lahore (A Comparative Cross Sectional Study)Document5 paginiOccupational Stress in Physical Therapist Working As Clinician and Academician in Lahore (A Comparative Cross Sectional Study)International Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- Esforço, Recompensa e Saúde Mental Autorreferida Um Estudo de Simulação Sobre Viés de Afetividade NegativaDocument7 paginiEsforço, Recompensa e Saúde Mental Autorreferida Um Estudo de Simulação Sobre Viés de Afetividade NegativaRonald SilvaÎncă nu există evaluări
- MRK - Spring 2022 - PAD619 - 8 - MC190400105Document20 paginiMRK - Spring 2022 - PAD619 - 8 - MC190400105Rehman KhanÎncă nu există evaluări
- KQW 155Document6 paginiKQW 155Al FatihÎncă nu există evaluări
- Work-Related Stress and Health-Risks, Mechanisms and CountermeasuresDocument9 paginiWork-Related Stress and Health-Risks, Mechanisms and CountermeasuresMetiku DigieÎncă nu există evaluări
- IIIIIIIIIIIIIIIDocument7 paginiIIIIIIIIIIIIIIIIceu AmiraÎncă nu există evaluări
- Occupational Risk Factors of Work Stress and Family Life of On Site Workers Amidst Covid 19 Pandemic: Basis For Psychological Counseling and Intervention ProgramDocument34 paginiOccupational Risk Factors of Work Stress and Family Life of On Site Workers Amidst Covid 19 Pandemic: Basis For Psychological Counseling and Intervention ProgramInternational Journal of Innovative Science and Research Technology100% (1)
- IJISRT23JUN1512Document34 paginiIJISRT23JUN1512International Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- Physical Psychological and Occupational Consequences of Job Burnout - A Systematic Review of Prospective StudiesDocument29 paginiPhysical Psychological and Occupational Consequences of Job Burnout - A Systematic Review of Prospective StudiesPaola GuerraÎncă nu există evaluări
- 2 32 1633674466 6ijbmrdec20216Document14 pagini2 32 1633674466 6ijbmrdec20216TJPRC PublicationsÎncă nu există evaluări
- Factors of Growing Mental Health Issues of Employees at Workplace in Service Based IndustryDocument33 paginiFactors of Growing Mental Health Issues of Employees at Workplace in Service Based IndustryNeha JainÎncă nu există evaluări
- The Depression Anxiety Stress Scales (DASS) - Detecting Anxiety Disorder and Depression in Employees Absent From Work Because of Mental Health ProblemsDocument7 paginiThe Depression Anxiety Stress Scales (DASS) - Detecting Anxiety Disorder and Depression in Employees Absent From Work Because of Mental Health ProblemsTran Huong TraÎncă nu există evaluări
- Journal Homepage: - : Manuscript HistoryDocument8 paginiJournal Homepage: - : Manuscript HistoryIJAR JOURNALÎncă nu există evaluări
- KQZ 160Document7 paginiKQZ 160mey ariyantiniÎncă nu există evaluări
- BO Organizational Climate and Employee Mental Health Outcomes - A Systematic Review of Studies in Health Care OrganizationsDocument42 paginiBO Organizational Climate and Employee Mental Health Outcomes - A Systematic Review of Studies in Health Care OrganizationsFlorencia BravoÎncă nu există evaluări
- Psychological Resilience and Burnout Levels in OccDocument23 paginiPsychological Resilience and Burnout Levels in OccCarlos Miguel SumagueÎncă nu există evaluări
- Literature ReviewsDocument11 paginiLiterature ReviewsDarah Angel LustreÎncă nu există evaluări
- IB ThesisDocument21 paginiIB ThesisNazish ShahzadiÎncă nu există evaluări
- Psychological Stress Experienced by Health Care PersonnelDocument9 paginiPsychological Stress Experienced by Health Care PersonnelMaria João MendesÎncă nu există evaluări
- Journal Homepage: - : IntroductionDocument9 paginiJournal Homepage: - : IntroductionIJAR JOURNALÎncă nu există evaluări
- DassDocument6 paginiDassGiftaniaÎncă nu există evaluări
- State of Stress in Nursing and Technical Health Professions in MoroccoDocument8 paginiState of Stress in Nursing and Technical Health Professions in MoroccoIJAR JOURNALÎncă nu există evaluări
- Measuring Work-Related Psychosocial and Physical Risk Factors UsingDocument3 paginiMeasuring Work-Related Psychosocial and Physical Risk Factors UsingPamela Soto MenautÎncă nu există evaluări
- Jobstressdimension MSDs WorkDocument8 paginiJobstressdimension MSDs WorkcacaÎncă nu există evaluări
- 1 s2.0 S1876201821004536 MainDocument7 pagini1 s2.0 S1876201821004536 Mainwatch2303Încă nu există evaluări
- UntitledDocument50 paginiUntitleddongxing zhouÎncă nu există evaluări
- 1 HHVHVHKVMDocument9 pagini1 HHVHVHKVMCreative Brain Institute of PsychologyÎncă nu există evaluări
- 9Document10 pagini9Yeremias EdwinÎncă nu există evaluări
- Keywords:-Bullying Behavior, Conservation of Resources,: Defensive Silence Well-Being, NursesDocument7 paginiKeywords:-Bullying Behavior, Conservation of Resources,: Defensive Silence Well-Being, NursesInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- Rudra Dissertation ReportDocument32 paginiRudra Dissertation ReportRudra narayan ParidaÎncă nu există evaluări
- Epidemiological and Clinical Predictors of License For Health Care Due To MBDDocument10 paginiEpidemiological and Clinical Predictors of License For Health Care Due To MBDDavi BaaschÎncă nu există evaluări
- Dissertation On Occupational StressDocument4 paginiDissertation On Occupational StressBuySchoolPapersOnlinePhoenix100% (1)
- Mental Health and Injured Workers - Depressive Symptoms Linked To Delayed Work-ReturnsDocument3 paginiMental Health and Injured Workers - Depressive Symptoms Linked To Delayed Work-ReturnsJose GonzalezÎncă nu există evaluări
- Gunjan Warkade Synopsis EditedDocument7 paginiGunjan Warkade Synopsis EditedPankaj Hatwar100% (1)
- Stress and Burnout Syndrome Among Moroccan Medical Students: A Cross-Sectional StudyDocument9 paginiStress and Burnout Syndrome Among Moroccan Medical Students: A Cross-Sectional StudyIJAR JOURNALÎncă nu există evaluări
- Occupational StressDocument11 paginiOccupational StressعزمباكلجوتوانÎncă nu există evaluări
- Jsju 2 - Workload Stress ExhaustionDocument15 paginiJsju 2 - Workload Stress ExhaustionBasilius Redan WerangÎncă nu există evaluări
- Impact of Job Stress by Shahid HafeezDocument9 paginiImpact of Job Stress by Shahid HafeezShahid HafeezÎncă nu există evaluări
- Stress Professionnel Et Consommation de Substances Psychoactives Chez Les Travailleurs Dune Usine de Cablage Au MarocDocument8 paginiStress Professionnel Et Consommation de Substances Psychoactives Chez Les Travailleurs Dune Usine de Cablage Au MarocIJAR JOURNALÎncă nu există evaluări
- Articulo 1 - InglesDocument7 paginiArticulo 1 - InglesmbarrosoarangoÎncă nu există evaluări
- Table 6 - Journal Paper 6Document8 paginiTable 6 - Journal Paper 6Rouhollah ParvariÎncă nu există evaluări
- Literature Review of Job StressDocument4 paginiLiterature Review of Job Stressafmzeracmdvbfe100% (2)
- ANational Standardfor Psychosocial Safety ClimateDocument13 paginiANational Standardfor Psychosocial Safety ClimateJorge Gabriel Chan CoobÎncă nu există evaluări
- Psychosocial Safety Climate Development of The PSC 12Document32 paginiPsychosocial Safety Climate Development of The PSC 12Buvan NairÎncă nu există evaluări
- 10 1108 - Ijwhm 09 2018 0116Document14 pagini10 1108 - Ijwhm 09 2018 0116ambusamsubramaniamÎncă nu există evaluări
- Bullying en El Trabajo y Sintomas AnsiososDocument12 paginiBullying en El Trabajo y Sintomas AnsiososManuel BallesterosÎncă nu există evaluări
- Literature Review 1Document60 paginiLiterature Review 1Quratulain BilalÎncă nu există evaluări
- Administrative Science QuarterlyDocument48 paginiAdministrative Science Quarterlydjhx5vv2s8Încă nu există evaluări
- Relationships Among Occupational StressDocument9 paginiRelationships Among Occupational StressMiezah ElliasonÎncă nu există evaluări
- 15 Castelli, Heeb, Gulfi, Gutjahr (2015)Document9 pagini15 Castelli, Heeb, Gulfi, Gutjahr (2015)Pablo Ferrer GonzalezÎncă nu există evaluări
- Work EnviromentDocument6 paginiWork EnviromentMonica MuresanÎncă nu există evaluări
- Certificat: S Ent of Ivth M T R A Y S Fte O Ogy B NG Ore. H Und R On G N U Organ A Ion Durin The E A C 2 8Document71 paginiCertificat: S Ent of Ivth M T R A Y S Fte O Ogy B NG Ore. H Und R On G N U Organ A Ion Durin The E A C 2 8Chetana YadawadÎncă nu există evaluări
- Slide Marine Cadastre 2Document15 paginiSlide Marine Cadastre 2ajib KanekiÎncă nu există evaluări
- Righeimer ComplaintDocument45 paginiRigheimer ComplaintSarah BatchaÎncă nu există evaluări
- Roy II vs. Herbosa, G.R. No. 207946, November 22, 2016Document20 paginiRoy II vs. Herbosa, G.R. No. 207946, November 22, 2016Rina OlandoÎncă nu există evaluări
- Petitioner vs. vs. Respondents Nicanor S. Bautista Agaton D. Yaranon Bince, Sevilleja, Agsalud & AssociatesDocument9 paginiPetitioner vs. vs. Respondents Nicanor S. Bautista Agaton D. Yaranon Bince, Sevilleja, Agsalud & AssociatesBianca BÎncă nu există evaluări
- Group6 Business-Proposal Delivery AppDocument15 paginiGroup6 Business-Proposal Delivery AppNathaniel Karl Enin PulidoÎncă nu există evaluări
- Surimi Technology: Submitted To: Dr.A.K.Singh (Sr. Scientist) Submitted By: Rahul Kumar (M.Tech, DT, 1 Year)Document13 paginiSurimi Technology: Submitted To: Dr.A.K.Singh (Sr. Scientist) Submitted By: Rahul Kumar (M.Tech, DT, 1 Year)rahuldtc100% (2)
- Programming Essentials in PythonDocument23 paginiProgramming Essentials in PythonNabeel AmjadÎncă nu există evaluări
- แบบฝึกหัด subjuctiveDocument6 paginiแบบฝึกหัด subjuctiveรัฐพล ทองแตงÎncă nu există evaluări
- 19.2 - China Limits European ContactsDocument17 pagini19.2 - China Limits European ContactsEftichia KatopodiÎncă nu există evaluări
- Argumentative Essay-2Document4 paginiArgumentative Essay-2api-385385980Încă nu există evaluări
- Course Welcome and Overview ACADocument20 paginiCourse Welcome and Overview ACAAlmerÎncă nu există evaluări
- 7999 Cswdo Day CareDocument3 pagini7999 Cswdo Day CareCharles D. FloresÎncă nu există evaluări
- Click To Enlarge (The Skeptic's Annotated Bible, Hosea)Document11 paginiClick To Enlarge (The Skeptic's Annotated Bible, Hosea)Philip WellsÎncă nu există evaluări
- Hermle C42 ENDocument72 paginiHermle C42 ENKiril AngelovÎncă nu există evaluări
- 10 Ideas For ConversationDocument116 pagini10 Ideas For ConversationGreenLake36100% (1)
- Practical No 4Document5 paginiPractical No 4Mahin SarkarÎncă nu există evaluări
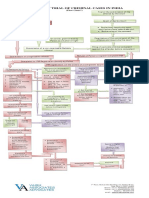
- Process of Trial of Criminal Cases in India (Flow Chart)Document1 paginăProcess of Trial of Criminal Cases in India (Flow Chart)Arun Hiro100% (1)
- Brief CVDocument6 paginiBrief CVDocument ReservedÎncă nu există evaluări
- MMDA v. Viron Transportation CoDocument3 paginiMMDA v. Viron Transportation CoTtlrpqÎncă nu există evaluări
- A Freudian Look Into Roger Waters' True Expressions in "The Wall."Document5 paginiA Freudian Look Into Roger Waters' True Expressions in "The Wall."Jacob Ritteman100% (1)
- MEM Companion Volume Implementation Guide - Release 1.1Document23 paginiMEM Companion Volume Implementation Guide - Release 1.1Stanley AlexÎncă nu există evaluări
- Microwave Oven: Instructions & Cooking GuideDocument38 paginiMicrowave Oven: Instructions & Cooking GuidethomaselandÎncă nu există evaluări
- Blood TestsDocument3 paginiBlood TestsMarycharinelle Antolin MolinaÎncă nu există evaluări
- The Value Relevance of Financial Statements and Their Impact On Stock PricesDocument18 paginiThe Value Relevance of Financial Statements and Their Impact On Stock Pricesanubha srivastavaÎncă nu există evaluări
- AIPT 2021 GuidelineDocument4 paginiAIPT 2021 GuidelineThsavi WijayasingheÎncă nu există evaluări
- Alternating Voltage and CurrentDocument41 paginiAlternating Voltage and CurrentKARTHIK LÎncă nu există evaluări
- English Full Book PaperDocument2 paginiEnglish Full Book PaperSaira BatoolÎncă nu există evaluări
- Wall Chart - Drying - How Wood Loses MoistureDocument1 paginăWall Chart - Drying - How Wood Loses MoistureXihuitl61100% (1)
- Effect of Intrinsic and Extrinsic Motivation On Academic PerformanceDocument11 paginiEffect of Intrinsic and Extrinsic Motivation On Academic Performancefarah ablayÎncă nu există evaluări