S-ar putea să vă placă și
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Upper Extremity Venous Protocol 14Document2 paginiUpper Extremity Venous Protocol 14api-349402240Încă nu există evaluări
- Upper Extremity Arterial Protocol 14Document3 paginiUpper Extremity Arterial Protocol 14api-349402240Încă nu există evaluări
- Renal Doppler Protocol 14 1Document4 paginiRenal Doppler Protocol 14 1api-349402240100% (1)
- Mesenteric Doppler Protocol 14Document2 paginiMesenteric Doppler Protocol 14api-349402240Încă nu există evaluări
- Lower Extremity Venous Protocol 14Document3 paginiLower Extremity Venous Protocol 14api-349474075Încă nu există evaluări
- Lower Extremity Arterial Protocol 14 1Document2 paginiLower Extremity Arterial Protocol 14 1api-3494022400% (1)
- Lower Extremity Venous Incompetence Protcol 14Document5 paginiLower Extremity Venous Incompetence Protcol 14api-349402240Încă nu există evaluări
- Adult Echocardiography Protocol 14 2Document10 paginiAdult Echocardiography Protocol 14 2api-349402240Încă nu există evaluări
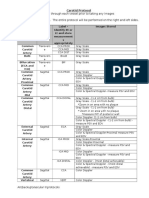
- Carotid Protocol 14 1Document4 paginiCarotid Protocol 14 1api-349402240Încă nu există evaluări
- Allen Test Protocol 14 1Document2 paginiAllen Test Protocol 14 1api-349402240Încă nu există evaluări
- Scrotum Protocol 14Document2 paginiScrotum Protocol 14api-349402240Încă nu există evaluări
- Pediatric Spine 14Document2 paginiPediatric Spine 14api-349402240Încă nu există evaluări
- Fetal Echocardiogram ProtocolDocument4 paginiFetal Echocardiogram Protocolapi-349402240Încă nu există evaluări
- Abdomen ProtocolDocument8 paginiAbdomen Protocolapi-349474075Încă nu există evaluări
- Liver Protocol 14 1Document5 paginiLiver Protocol 14 1api-349402240Încă nu există evaluări
- Appendix Protocol 14 1Document2 paginiAppendix Protocol 14 1api-349402240Încă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Q1 - Weekly Test 4 - SSESDocument7 paginiQ1 - Weekly Test 4 - SSESJoan AgranoÎncă nu există evaluări
- 113 DigestionDocument22 pagini113 DigestionCath DetoperezÎncă nu există evaluări
- Kolar 2014Document6 paginiKolar 2014Arnold Barra100% (1)
- Digestive System Parts PacketDocument2 paginiDigestive System Parts PacketRusherÎncă nu există evaluări
- Evaluation of The Lumbar Multifidus in Rowers During Espinal Estabilizacion ExercisesDocument7 paginiEvaluation of The Lumbar Multifidus in Rowers During Espinal Estabilizacion ExercisesAline KreiÎncă nu există evaluări
- Hepatorenal SyndromeDocument6 paginiHepatorenal SyndromeAditi Ujjawal0% (1)
- NGNTestPacket 110322Document64 paginiNGNTestPacket 110322romeliza romeliza0% (1)
- English Homework 4Document2 paginiEnglish Homework 4Teodora TanaseÎncă nu există evaluări
- Abdominal Examination OSCE GuideDocument30 paginiAbdominal Examination OSCE Guideزياد سعيدÎncă nu există evaluări
- ST 32Document1 paginăST 32ray72roÎncă nu există evaluări
- LECTURE 2 Urinary System - Histology HB II 2023Document79 paginiLECTURE 2 Urinary System - Histology HB II 2023Emmanuel AssopiahÎncă nu există evaluări
- Act 2 - DIgestive SystemDocument37 paginiAct 2 - DIgestive Systemisabellamarie.castillo.crsÎncă nu există evaluări
- Anatomi Dan Fisiologi GinjalDocument32 paginiAnatomi Dan Fisiologi GinjalAlamul Huda100% (1)
- Medical Symptoms: A Visual GuideDocument258 paginiMedical Symptoms: A Visual GuideJason Peters100% (11)
- Digestive System ExamDocument9 paginiDigestive System ExamChris RosarioÎncă nu există evaluări
- Anatomy of The LiverDocument34 paginiAnatomy of The LiverOmiko Fidelis NnamdiÎncă nu există evaluări
- Frog Dissection WorksheetDocument7 paginiFrog Dissection WorksheetJoanna AcuñaÎncă nu există evaluări
- Abdominal ExamDocument21 paginiAbdominal ExamnouraÎncă nu există evaluări
- FIU - Thoracic and Lumbar Spine Clinical EvaluationDocument51 paginiFIU - Thoracic and Lumbar Spine Clinical Evaluationmursyid nasruddinÎncă nu există evaluări
- Lumbar Core StrenghtDocument8 paginiLumbar Core StrenghtMattia BressanÎncă nu există evaluări
- Antenatal ExercisesDocument11 paginiAntenatal ExercisesRashmi C S0% (1)
- Science8 Q4-Module 1Document16 paginiScience8 Q4-Module 1Lovelyjoy MarianoÎncă nu există evaluări
- Morphing Nose Cone - 2Document10 paginiMorphing Nose Cone - 2Naufal PutraÎncă nu există evaluări
- Oesophagus, Stomach-Fundus & Pylorus: Dr. Makarchuk IrynaDocument35 paginiOesophagus, Stomach-Fundus & Pylorus: Dr. Makarchuk IrynaSerious LeoÎncă nu există evaluări
- Abdominal Wall DefectsDocument20 paginiAbdominal Wall DefectsxylomiteÎncă nu există evaluări
- Peritoneum - Dr. QuratulainDocument40 paginiPeritoneum - Dr. QuratulainWajahat FaizÎncă nu există evaluări
- Prof. Joseph Bahian Abang,: Ahse, BSN, RN, Man (C)Document67 paginiProf. Joseph Bahian Abang,: Ahse, BSN, RN, Man (C)Yucef Bahian-AbangÎncă nu există evaluări
- Reflux Disease (Nerd) Di Rsud Dr. Soetomo SurabayaDocument6 paginiReflux Disease (Nerd) Di Rsud Dr. Soetomo SurabayaFajriÎncă nu există evaluări
- Digestive SystemDocument6 paginiDigestive SystemDorence SimuntalaÎncă nu există evaluări
- Hernia Surgery SimplifiedDocument221 paginiHernia Surgery SimplifiedDr Saad ur Rehman100% (2)