S-ar putea să vă placă și
- The Prevention and Treatment of Disease with a Plant-Based Diet Volume 2: Evidence-based articles to guide the physicianDe la EverandThe Prevention and Treatment of Disease with a Plant-Based Diet Volume 2: Evidence-based articles to guide the physicianÎncă nu există evaluări
- Case 18-2017 - An 11-Year-Old Girl With Difficulty Eating After A Choking Incident-2017Document10 paginiCase 18-2017 - An 11-Year-Old Girl With Difficulty Eating After A Choking Incident-2017Juan ParedesÎncă nu există evaluări
- Understanding Diabetes for Action: Rethinking How You Handle Diabetes a Holistic ApproachDe la EverandUnderstanding Diabetes for Action: Rethinking How You Handle Diabetes a Holistic ApproachÎncă nu există evaluări
- Cerebral Palsy A Clinico-Social Case ReportDocument5 paginiCerebral Palsy A Clinico-Social Case ReportNovie AstiniÎncă nu există evaluări
- Alcohol, Drugs and Medication in Pregnancy: The Long Term Outcome for the ChildDe la EverandAlcohol, Drugs and Medication in Pregnancy: The Long Term Outcome for the ChildPhilip M PreeceEvaluare: 1 din 5 stele1/5 (1)
- Monek Case StudyDocument24 paginiMonek Case StudyashnairafatimamaulanaÎncă nu există evaluări
- Essential Medical Disorders of the Stomach and Small Intestine: A Clinical CasebookDe la EverandEssential Medical Disorders of the Stomach and Small Intestine: A Clinical CasebookÎncă nu există evaluări
- Prader-Willi SyndromeDocument17 paginiPrader-Willi Syndromejazzy tonezÎncă nu există evaluări
- Case Study PaediatricsDocument8 paginiCase Study PaediatricsDaudÎncă nu există evaluări
- Case Study Uro FinalDocument44 paginiCase Study Uro FinalDan Ataniel EnsaladaÎncă nu există evaluări
- ApproachpatientpwDocument8 paginiApproachpatientpwPatricia Rearte CarvalhoÎncă nu există evaluări
- A Case Study of An Older Adult With Severe Anemia Refusing Blood TransfusionDocument7 paginiA Case Study of An Older Adult With Severe Anemia Refusing Blood TransfusionКристофер траукоÎncă nu există evaluări
- Ectopic Pregnancy Case StudyDocument69 paginiEctopic Pregnancy Case StudyMo-nhica Luise AlundayÎncă nu există evaluări
- Treatment of Feeding Disorders in Children With Down SyndromeDocument13 paginiTreatment of Feeding Disorders in Children With Down SyndromeDaniela Aguirre GonzálezÎncă nu există evaluări
- University of Northern PhilippinesDocument30 paginiUniversity of Northern PhilippinesClaudine JaramilloÎncă nu există evaluări
- A Case Study of Epidural HematomaDocument27 paginiA Case Study of Epidural HematomaNeil GoÎncă nu există evaluări
- A Care Study ON Normal Spontaneous Vaginal DeliveryDocument35 paginiA Care Study ON Normal Spontaneous Vaginal DeliveryCharlskin LetzÎncă nu există evaluări
- Case 36-2004: A 23-Day-Old Infant With Hypospadias and Failure To ThriveDocument8 paginiCase 36-2004: A 23-Day-Old Infant With Hypospadias and Failure To ThriveGaniahUtamiÎncă nu există evaluări
- Dengue Case StudyDocument20 paginiDengue Case Studyjohn jumborockÎncă nu există evaluări
- CKD (F&e)Document110 paginiCKD (F&e)Al-nazer Azer Al100% (1)
- Revised Ischemic Stroke 3Document22 paginiRevised Ischemic Stroke 3Alayza Joy GasmenÎncă nu există evaluări
- Acute Hypotonia in An Infant (2017)Document3 paginiAcute Hypotonia in An Infant (2017)nikos.alexandrÎncă nu există evaluări
- A Novel Psychiatric Phenotype of Chromosome 4q DelDocument10 paginiA Novel Psychiatric Phenotype of Chromosome 4q DelgroyonroyÎncă nu există evaluări
- Inguinal Hernia: Related Learning ExperienceDocument29 paginiInguinal Hernia: Related Learning Experience'mYk FavilaÎncă nu există evaluări
- Original Study: Gynecologic Issues of Adolescents With Down Syndrome, Autism, and Cerebral PalsyDocument5 paginiOriginal Study: Gynecologic Issues of Adolescents With Down Syndrome, Autism, and Cerebral PalsyZubaidah HassanÎncă nu există evaluări
- Model Paper 4Document22 paginiModel Paper 4Mobin Ur Rehman KhanÎncă nu există evaluări
- Case English 1 - NDI Edit 220419Document24 paginiCase English 1 - NDI Edit 220419syongebobÎncă nu există evaluări
- Ruth H. Stonestreet, PH.D., CCC SLP Jessie L. Nelson, B.S.Ed Corine C. Myers Jennings, PH.D., CCC SLP Valdosta State University Valdosta, GeorgiaDocument30 paginiRuth H. Stonestreet, PH.D., CCC SLP Jessie L. Nelson, B.S.Ed Corine C. Myers Jennings, PH.D., CCC SLP Valdosta State University Valdosta, Georgialily147dÎncă nu există evaluări
- Failure To Thrive, Hyponatremia, and Hyperkalemia in A NeonateDocument6 paginiFailure To Thrive, Hyponatremia, and Hyperkalemia in A NeonateMarselya GaniÎncă nu există evaluări
- Presentation of CaseDocument10 paginiPresentation of CaseAmazonJambiÎncă nu există evaluări
- Scurvy: A Case Report On A Child With AutismDocument5 paginiScurvy: A Case Report On A Child With AutismReuben JosephÎncă nu există evaluări
- Case Study 1 1Document21 paginiCase Study 1 1Melody DoriaÎncă nu există evaluări
- F2F MeaslesDocument7 paginiF2F MeaslesMichelle Gliselle Guinto MallareÎncă nu există evaluări
- Lapkas Anak (Prof Dr. Hj. Bidasari)Document74 paginiLapkas Anak (Prof Dr. Hj. Bidasari)Maral Bimanti Febrilina100% (1)
- Nursing Care Plan for Mrs. Yolanda Yambut BenavidezDocument8 paginiNursing Care Plan for Mrs. Yolanda Yambut BenavidezRafi LabÎncă nu există evaluări
- Delirium - Erica NewkirkDocument16 paginiDelirium - Erica NewkirkSalbia RiasatÎncă nu există evaluări
- Vehicular AccidentDocument9 paginiVehicular AccidentCharm TanyaÎncă nu există evaluări
- CP On Pre-EclampsiaDocument152 paginiCP On Pre-Eclampsiakathy100% (2)
- Practice Parameters: Assessment and Management of Patients in The Persistent Vegetative State (Summary Statement)Document7 paginiPractice Parameters: Assessment and Management of Patients in The Persistent Vegetative State (Summary Statement)mr.anggaardiantoÎncă nu există evaluări
- Neonatal Vomiting Due to Pyloric Stenosis and Congenital Nephrotic SyndromeDocument5 paginiNeonatal Vomiting Due to Pyloric Stenosis and Congenital Nephrotic SyndromeHanny RusliÎncă nu există evaluări
- Hyperemesis GravidarumDocument5 paginiHyperemesis GravidarumJeg B. Israel Jr.Încă nu există evaluări
- Lumbar Compression FractureDocument47 paginiLumbar Compression FractureAngelie Sanchez50% (2)
- POWERPOINTDocument55 paginiPOWERPOINTJosie Enad Purlares CelyonÎncă nu există evaluări
- hnf41 Revised by Lau - To Be PrintDocument62 paginihnf41 Revised by Lau - To Be PrintJessa EsguerraÎncă nu există evaluări
- Calculus CholecystitisDocument48 paginiCalculus CholecystitisEdderlyn LamarcaÎncă nu există evaluări
- Case StudyDocument12 paginiCase Studyapi-401961702Încă nu există evaluări
- Pedsinreview 2021005211Document3 paginiPedsinreview 2021005211Claudio MontiÎncă nu există evaluări
- Case Analysis on Cholecystectomy CareDocument18 paginiCase Analysis on Cholecystectomy CareAllyssa AnastacioÎncă nu există evaluări
- Case Analysis on Cholecystectomy CareDocument18 paginiCase Analysis on Cholecystectomy CareAllyssa AnastacioÎncă nu există evaluări
- Case Analysis on Cholecystectomy CareDocument18 paginiCase Analysis on Cholecystectomy CareAllyssa AnastacioÎncă nu există evaluări
- Client Nursing Care Plan for CholecystolithiasisDocument9 paginiClient Nursing Care Plan for CholecystolithiasisBelen SoleroÎncă nu există evaluări
- Idiopathic Thrombocytopenic PurpuraDocument45 paginiIdiopathic Thrombocytopenic PurpuraOhnesan Medina PerezÎncă nu există evaluări
- 1 Professional Experience Analysis EssayDocument12 pagini1 Professional Experience Analysis EssayGurjot KaurÎncă nu există evaluări
- 28099453C Case Study 3Document27 pagini28099453C Case Study 3Alice HuiiÎncă nu există evaluări
- Pediatrics 2015Document9 paginiPediatrics 2015Randy PrayogoÎncă nu există evaluări
- CHOLEDOCHOLITHIASISDocument38 paginiCHOLEDOCHOLITHIASISPrecious Cofreros100% (3)
- American Academy of Pediatrics Metabolic Disorders 2014 Practice TestDocument43 paginiAmerican Academy of Pediatrics Metabolic Disorders 2014 Practice TestPrabu KumarÎncă nu există evaluări
- Lumbar Compression Fracture: A Case StudyDocument46 paginiLumbar Compression Fracture: A Case StudyOlivia SolomonÎncă nu există evaluări
- CP (Sub-Grp)Document79 paginiCP (Sub-Grp)Pamela laquindanumÎncă nu există evaluări
- Letters To The Editor: ReferenceDocument2 paginiLetters To The Editor: ReferenceEvelina Lestari NapitupuluÎncă nu există evaluări
- Atresia Biliaris PDFDocument9 paginiAtresia Biliaris PDFIrenaÎncă nu există evaluări
- RSDK Thalassemia Integrated Center 2Document24 paginiRSDK Thalassemia Integrated Center 2irenaÎncă nu există evaluări
- Do All Chldren With CAP Need Blood CultureDocument5 paginiDo All Chldren With CAP Need Blood CultureIrenaÎncă nu există evaluări
- 10 - 258sepsis Neonatorum Awitan DiniDocument4 pagini10 - 258sepsis Neonatorum Awitan DiniIrenaÎncă nu există evaluări
- TRANSLATED Case Report ThalasemiaDocument56 paginiTRANSLATED Case Report ThalasemiaIrenaÎncă nu există evaluări
- Efficacy and Safety of Vitamin D SupplementationDocument8 paginiEfficacy and Safety of Vitamin D SupplementationIrenaÎncă nu există evaluări
- A Critical Perspective On Trophic Feeding.1Document2 paginiA Critical Perspective On Trophic Feeding.1IrenaÎncă nu există evaluări
- Specific Nutritional Problems in Acute Kidney Injury, Treated WithDocument7 paginiSpecific Nutritional Problems in Acute Kidney Injury, Treated WithIrenaÎncă nu există evaluări
- Case ReportSevere Form of Hemolytic-Uremic SyndromeDocument9 paginiCase ReportSevere Form of Hemolytic-Uremic SyndromeIrenaÎncă nu există evaluări
- Do All Chldren With CAP Need Blood CultureDocument5 paginiDo All Chldren With CAP Need Blood CultureIrenaÎncă nu există evaluări
- Antibiotik SepsisDocument22 paginiAntibiotik SepsisIrenaÎncă nu există evaluări
- Childhood MedulloblastmaDocument17 paginiChildhood MedulloblastmaIrenaÎncă nu există evaluări
- Ment ZerDocument7 paginiMent ZerIrenaÎncă nu există evaluări
- Iron Overload in Transfusion-DependentDocument2 paginiIron Overload in Transfusion-DependentIrena100% (2)
- Chang2014 KappaDocument17 paginiChang2014 KappaIrenaÎncă nu există evaluări
- Impact of Kasai Portoenterostomy On LiverDocument6 paginiImpact of Kasai Portoenterostomy On LiverIrenaÎncă nu există evaluări
- Pertussis Grade Table 2Document4 paginiPertussis Grade Table 2IrenaÎncă nu există evaluări
- Cow's Milk AllergyDocument26 paginiCow's Milk AllergyIrenaÎncă nu există evaluări
- Tugas Jurnal Junior Stase RespirologiDocument44 paginiTugas Jurnal Junior Stase RespirologiIrenaÎncă nu există evaluări
- Aspiration Pneumonia With Special Reference ToDocument10 paginiAspiration Pneumonia With Special Reference ToIrenaÎncă nu există evaluări
- Dialysis Disequilibrium SyndromeDocument7 paginiDialysis Disequilibrium Syndromesatyagraha84Încă nu există evaluări
- Quantitative Aspiration During Sleep inDocument7 paginiQuantitative Aspiration During Sleep inIrenaÎncă nu există evaluări
- ASD, National Mental HealthDocument8 paginiASD, National Mental HealthIrenaÎncă nu există evaluări
- Anatomic Features of Growth Failure inDocument10 paginiAnatomic Features of Growth Failure inIrenaÎncă nu există evaluări
- Multimodal Learning Through Media PDFDocument24 paginiMultimodal Learning Through Media PDFIrenaÎncă nu există evaluări
- (Translational Neuroscience) Multisensory Integration and Neuroplasticity in The Human Cerebral CortexDocument12 pagini(Translational Neuroscience) Multisensory Integration and Neuroplasticity in The Human Cerebral CortexIrenaÎncă nu există evaluări
- Mid-Term Outcomes After Percutaneous Closure of The Secundum AtrialDocument8 paginiMid-Term Outcomes After Percutaneous Closure of The Secundum AtrialIrenaÎncă nu există evaluări
- Effectiveness of Multisensory Stimulation in ManagingDocument11 paginiEffectiveness of Multisensory Stimulation in ManagingIrenaÎncă nu există evaluări
- A Meta-Analysis of Interventions On Challenging BehaviourDocument16 paginiA Meta-Analysis of Interventions On Challenging BehaviourIrenaÎncă nu există evaluări
- A Meta-Analysis of Interventions On Challenging BehaviourDocument16 paginiA Meta-Analysis of Interventions On Challenging BehaviourIrenaÎncă nu există evaluări
- Psychopathology and Developmental InfluencesDocument28 paginiPsychopathology and Developmental InfluencesJoy AlexisÎncă nu există evaluări
- Nervous System WebquestDocument6 paginiNervous System Webquestapi-294104473Încă nu există evaluări
- Regeneration of The Heart: Matthew L. Steinhauser, Richard T. LeeDocument12 paginiRegeneration of The Heart: Matthew L. Steinhauser, Richard T. LeeᄋÎncă nu există evaluări
- Understanding Nodular PrurigoDocument5 paginiUnderstanding Nodular Prurigoranz ibonkÎncă nu există evaluări
- Basic Molecular Genetic Mechanisms: (Part 3)Document35 paginiBasic Molecular Genetic Mechanisms: (Part 3)ofirÎncă nu există evaluări
- Case Conceptualization BowenDocument2 paginiCase Conceptualization BowenJovencio Marquez0% (1)
- Harr. Cap 114Document7 paginiHarr. Cap 114tkovats.lopes2Încă nu există evaluări
- Bioactive Natural Products Opportunities and Challenges in MedicinalDocument695 paginiBioactive Natural Products Opportunities and Challenges in Medicinalney.barbosaÎncă nu există evaluări
- Acid-Base Balance in AnimalsDocument24 paginiAcid-Base Balance in AnimalselsaÎncă nu există evaluări
- Rheumatoid ArthritisDocument38 paginiRheumatoid ArthritisOlga GoryachevaÎncă nu există evaluări
- Мотивационное письмо образецDocument4 paginiМотивационное письмо образецOncampus - ваш гид по образованию за рубежом75% (4)
- Jurnal Tonsil Limfoma Non HodgkinDocument5 paginiJurnal Tonsil Limfoma Non HodgkinAhmad RamadhanuÎncă nu există evaluări
- Guidelines for Microbiology Specimen ProcessingDocument48 paginiGuidelines for Microbiology Specimen ProcessingAl- ImanuddinÎncă nu există evaluări
- B.pharm SyllabusDocument50 paginiB.pharm SyllabusSunil SharmaÎncă nu există evaluări
- Criminal Behavior Genre DraftDocument6 paginiCriminal Behavior Genre Draftapi-309159739Încă nu există evaluări
- Application For Job: Date: 17/05/2023Document7 paginiApplication For Job: Date: 17/05/2023Bikila RusiÎncă nu există evaluări
- Transfusion 2015 ChapuyDocument11 paginiTransfusion 2015 ChapuyNedelcu CarmenÎncă nu există evaluări
- Gen Bio 1 - Mitosis and MeiosisDocument22 paginiGen Bio 1 - Mitosis and MeiosisQuiel Tangonan Jr.Încă nu există evaluări
- About Inflammation and InfectionDocument2 paginiAbout Inflammation and InfectionHAZRULÎncă nu există evaluări
- Proteomics: Technologies and Global MarketsDocument5 paginiProteomics: Technologies and Global MarketsBCC ResearchÎncă nu există evaluări
- Superparamagnetism: Limits and ApplicationsDocument7 paginiSuperparamagnetism: Limits and ApplicationsNguyen VuÎncă nu există evaluări
- Functions of Blood and ComponentsDocument15 paginiFunctions of Blood and ComponentsayuÎncă nu există evaluări
- NCP For Ectopic PregnancyDocument4 paginiNCP For Ectopic PregnancyClarissa_Dante_735850% (4)
- Cmca Lec Prelim ReviewerDocument26 paginiCmca Lec Prelim ReviewerCrystal MiranaÎncă nu există evaluări
- AlbinismDocument5 paginiAlbinismAde BuligaÎncă nu există evaluări
- Cellular Nutrition - The Key to Preventing Oxidative StressDocument4 paginiCellular Nutrition - The Key to Preventing Oxidative StressFxStuntDriver100% (3)
- Omics-Based On Science, Technology, and Applications OmicsDocument22 paginiOmics-Based On Science, Technology, and Applications OmicsAlex Yalew0% (1)
- ( ( ( ( ( ( ( ( ( ( ( ( ( ( ( - Clinical Trial - (Publication Type) or - Clinical Trials - PubMed - NCBI45Document23 pagini( ( ( ( ( ( ( ( ( ( ( ( ( ( ( - Clinical Trial - (Publication Type) or - Clinical Trials - PubMed - NCBI45Túlio Martins OliveiraÎncă nu există evaluări
- Current GM Crops & Transgenic AnimalsDocument12 paginiCurrent GM Crops & Transgenic AnimalsJhayce Christian S. CapanayanÎncă nu există evaluări
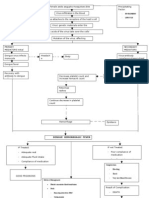
- Pathophysio DHF EDITEDDocument3 paginiPathophysio DHF EDITEDricmichael100% (1)
- The Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyDe la EverandThe Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyEvaluare: 5 din 5 stele5/5 (1)
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisDe la EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisEvaluare: 3 din 5 stele3/5 (2)
- Keto Friendly Recipes: Easy Keto For Busy PeopleDe la EverandKeto Friendly Recipes: Easy Keto For Busy PeopleEvaluare: 3.5 din 5 stele3.5/5 (2)
- Instant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookDe la EverandInstant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookEvaluare: 3.5 din 5 stele3.5/5 (2)
- Allen Carr's Easy Way for Women to Lose Weight: The original Easyway methodDe la EverandAllen Carr's Easy Way for Women to Lose Weight: The original Easyway methodEvaluare: 4.5 din 5 stele4.5/5 (18)
- Summary of Mary Claire Haver's The Galveston DietDe la EverandSummary of Mary Claire Haver's The Galveston DietEvaluare: 5 din 5 stele5/5 (1)
- Forever Strong: A New, Science-Based Strategy for Aging WellDe la EverandForever Strong: A New, Science-Based Strategy for Aging WellÎncă nu există evaluări
- Body Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomDe la EverandBody Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomEvaluare: 4 din 5 stele4/5 (1)
- Glucose Goddess Method: A 4-Week Guide to Cutting Cravings, Getting Your Energy Back, and Feeling AmazingDe la EverandGlucose Goddess Method: A 4-Week Guide to Cutting Cravings, Getting Your Energy Back, and Feeling AmazingEvaluare: 5 din 5 stele5/5 (59)
- The Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsDe la EverandThe Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsEvaluare: 4 din 5 stele4/5 (49)
- The Fast800 Diet: Discover the Ideal Fasting Formula to Shed Pounds, Fight Disease, and Boost Your Overall HealthDe la EverandThe Fast800 Diet: Discover the Ideal Fasting Formula to Shed Pounds, Fight Disease, and Boost Your Overall HealthEvaluare: 5 din 5 stele5/5 (37)
- Hungry for Change: Ditch the Diets, Conquer the Cravings, and Eat Your Way to Lifelong HealthDe la EverandHungry for Change: Ditch the Diets, Conquer the Cravings, and Eat Your Way to Lifelong HealthEvaluare: 4 din 5 stele4/5 (7)
- Happy Gut: The Cleansing Program to Help You Lose Weight, Gain Energy, and Eliminate PainDe la EverandHappy Gut: The Cleansing Program to Help You Lose Weight, Gain Energy, and Eliminate PainEvaluare: 3.5 din 5 stele3.5/5 (6)
- Proteinaholic: How Our Obsession with Meat Is Killing Us and What We Can Do About ItDe la EverandProteinaholic: How Our Obsession with Meat Is Killing Us and What We Can Do About ItEvaluare: 4.5 din 5 stele4.5/5 (19)
- How to Be Well: The 6 Keys to a Happy and Healthy LifeDe la EverandHow to Be Well: The 6 Keys to a Happy and Healthy LifeEvaluare: 5 din 5 stele5/5 (1)
- Eat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouDe la EverandEat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouÎncă nu există evaluări
- Metabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeDe la EverandMetabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeÎncă nu există evaluări
- The Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthDe la EverandThe Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthÎncă nu există evaluări
- Grit & Grace: Train the Mind, Train the Body, Own Your LifeDe la EverandGrit & Grace: Train the Mind, Train the Body, Own Your LifeEvaluare: 4 din 5 stele4/5 (3)
- Lose Weight by Eating: 130 Amazing Clean-Eating Makeovers for Guilt-Free Comfort FoodDe la EverandLose Weight by Eating: 130 Amazing Clean-Eating Makeovers for Guilt-Free Comfort FoodEvaluare: 2 din 5 stele2/5 (1)
- Rapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreDe la EverandRapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreEvaluare: 5 din 5 stele5/5 (17)
- The Intuitive Eating Workbook: 10 Principles for Nourishing a Healthy Relationship with FoodDe la EverandThe Intuitive Eating Workbook: 10 Principles for Nourishing a Healthy Relationship with FoodEvaluare: 4.5 din 5 stele4.5/5 (20)
- Ultrametabolism: The Simple Plan for Automatic Weight LossDe la EverandUltrametabolism: The Simple Plan for Automatic Weight LossEvaluare: 4.5 din 5 stele4.5/5 (28)
- The Raw Food Detox Diet: The Five-Step Plan for Vibrant Health and Maximum Weight LossDe la EverandThe Raw Food Detox Diet: The Five-Step Plan for Vibrant Health and Maximum Weight LossEvaluare: 4 din 5 stele4/5 (22)
- The Whole Body Reset: Your Weight-Loss Plan for a Flat Belly, Optimum Health & a Body You'll Love at Midlife and BeyondDe la EverandThe Whole Body Reset: Your Weight-Loss Plan for a Flat Belly, Optimum Health & a Body You'll Love at Midlife and BeyondEvaluare: 4.5 din 5 stele4.5/5 (28)
- Power Souping: 3-Day Detox, 3-Week Weight-Loss PlanDe la EverandPower Souping: 3-Day Detox, 3-Week Weight-Loss PlanEvaluare: 3.5 din 5 stele3.5/5 (3)
- The Longevity Plan: Seven Life-Transforming Lessons from Ancient ChinaDe la EverandThe Longevity Plan: Seven Life-Transforming Lessons from Ancient ChinaÎncă nu există evaluări
- Think Yourself Thin: A 30-Day Guide to Permanent Weight LossDe la EverandThink Yourself Thin: A 30-Day Guide to Permanent Weight LossEvaluare: 4.5 din 5 stele4.5/5 (22)