S-ar putea să vă placă și
- First Guide C - Rev2Document8 paginiFirst Guide C - Rev2Suraj PathakÎncă nu există evaluări
- Medical Education in Pulmonary, Critical Care, and Sleep Medicine: Advanced Concepts and StrategiesDe la EverandMedical Education in Pulmonary, Critical Care, and Sleep Medicine: Advanced Concepts and StrategiesPatricia A. KritekÎncă nu există evaluări
- Simulation-Based Learning: Just Like The Real Thing: Go ToDocument10 paginiSimulation-Based Learning: Just Like The Real Thing: Go ToClaude Geoffrey escanillaÎncă nu există evaluări
- Running Head:Simulation-Based EducationDocument9 paginiRunning Head:Simulation-Based EducationSana RazaÎncă nu există evaluări
- Nursing Students' Achievement in Normal Labor: Impact of Simulation ModulesDocument6 paginiNursing Students' Achievement in Normal Labor: Impact of Simulation ModulesMd Salah Uddin RajibÎncă nu există evaluări
- Texto 3Document10 paginiTexto 3Omid Ernesto Chahuaris ChoqueÎncă nu există evaluări
- Writing A Simulation Scenario: A Step-By-Step Guide: Deborah Bambini, PHD, WHNP-BC, Cne, ChseDocument10 paginiWriting A Simulation Scenario: A Step-By-Step Guide: Deborah Bambini, PHD, WHNP-BC, Cne, ChseEsteban RamosÎncă nu există evaluări
- Simulation in Nursing EducationDocument12 paginiSimulation in Nursing EducationGaje SinghÎncă nu există evaluări
- SimulationDocument2 paginiSimulationVin Mamuric Meneses100% (1)
- Simulation White Paper2Document147 paginiSimulation White Paper2Matet SantosidadÎncă nu există evaluări
- Southern Luzon State University College of Allied Medicine Lucban, QuezonDocument4 paginiSouthern Luzon State University College of Allied Medicine Lucban, Quezonmelanie perezÎncă nu există evaluări
- Steps of SimulationDocument13 paginiSteps of Simulationsubashik100% (1)
- Types of Simulation in Nursing EducationDocument7 paginiTypes of Simulation in Nursing EducationKarl RobleÎncă nu există evaluări
- Lesson 12 MODELS OF CLINICAL TEACHINGDocument57 paginiLesson 12 MODELS OF CLINICAL TEACHINGwedad jumaÎncă nu există evaluări
- Clinical Simulation: Changing The Landscape of Nursing EducationDocument5 paginiClinical Simulation: Changing The Landscape of Nursing EducationKenneth Myro GarciaÎncă nu există evaluări
- Simulation PPT MDocument23 paginiSimulation PPT MPooja100% (1)
- Clinical Skills CentreDocument12 paginiClinical Skills Centreد.احمد عبدالكريمÎncă nu există evaluări
- Clincial Simulation ScenariosDocument8 paginiClincial Simulation ScenariosV_RNÎncă nu există evaluări
- High-Fidelity Simulation Effects On CPR Knowledge, Skills, Acquisition, and Retention in Nursing StudentsDocument7 paginiHigh-Fidelity Simulation Effects On CPR Knowledge, Skills, Acquisition, and Retention in Nursing StudentsMuhammad HidirÎncă nu există evaluări
- 1761-Article Text-3778-1-10-20180120 PDFDocument12 pagini1761-Article Text-3778-1-10-20180120 PDFArianna Jasmine MabungaÎncă nu există evaluări
- Simulation in Nursing EducationDocument9 paginiSimulation in Nursing EducationbldewnaÎncă nu există evaluări
- Simulation in Nursing EducationDocument8 paginiSimulation in Nursing EducationbldewnaÎncă nu există evaluări
- Landasan TeoriDocument3 paginiLandasan TeoriSri WahyuÎncă nu există evaluări
- How To Teach Practical SkillsDocument16 paginiHow To Teach Practical SkillsShazia Farman Ali QaziÎncă nu există evaluări
- Simulation in Nursing EducationDocument7 paginiSimulation in Nursing EducationGaje SinghÎncă nu există evaluări
- 90-24 Patient SimulationDocument6 pagini90-24 Patient SimulationYlron John TaparÎncă nu există evaluări
- Healthcare Education With Virtual-World SimulationDocument11 paginiHealthcare Education With Virtual-World SimulationDaniel MelloÎncă nu există evaluări
- Innovation Center: Simulation To Prepare Graduate Nursing Students For Clinical Faculty RoleDocument3 paginiInnovation Center: Simulation To Prepare Graduate Nursing Students For Clinical Faculty RoleGisele Elise MeninÎncă nu există evaluări
- Effectiveness of Simulation-Based Nursing Education Depending On Fidelity: A Meta-AnalysisDocument8 paginiEffectiveness of Simulation-Based Nursing Education Depending On Fidelity: A Meta-AnalysisSydney FeldmanÎncă nu există evaluări
- Nursing Skills Laboratory As Milieu of Clinical Learning and PracticeDocument6 paginiNursing Skills Laboratory As Milieu of Clinical Learning and Practicetiana raditaÎncă nu există evaluări
- CHAPTER 7 Clinical TeachingDocument3 paginiCHAPTER 7 Clinical TeachingKim Angelo del CastilloÎncă nu există evaluări
- Simulation-Based Medical Education: Time For A Pedagogical ShiftDocument5 paginiSimulation-Based Medical Education: Time For A Pedagogical ShiftAshish kumarÎncă nu există evaluări
- 1 PBDocument9 pagini1 PBAna Marie ZalunÎncă nu există evaluări
- Special Contributions Virtual Reality and Simulation: Training The Future Emergency PhysicianDocument9 paginiSpecial Contributions Virtual Reality and Simulation: Training The Future Emergency PhysicianOmid Ernesto Chahuaris ChoqueÎncă nu există evaluări
- Simulation in NursingDocument12 paginiSimulation in Nursingkateypark1485Încă nu există evaluări
- Alinier G. Med Teach. 2007 29Document9 paginiAlinier G. Med Teach. 2007 29Esteban RamosÎncă nu există evaluări
- Keele FrameworkDocument6 paginiKeele FrameworkNoreen PunjwaniÎncă nu există evaluări
- Research Namin Ni Karl and Carzi Sana Last NaDocument30 paginiResearch Namin Ni Karl and Carzi Sana Last Nakarlamper20Încă nu există evaluări
- A Cost-Effectiveness Analysis of Self-Debriefing Versus Instructor Debriefing For Simulated Crises in Perioperative Medicine in CanadaDocument7 paginiA Cost-Effectiveness Analysis of Self-Debriefing Versus Instructor Debriefing For Simulated Crises in Perioperative Medicine in CanadaKuba KozerskiÎncă nu există evaluări
- Nursing Simulation Scenarios - Preparing Tomorrow's Nurses, Today - Wolters KluwerDocument10 paginiNursing Simulation Scenarios - Preparing Tomorrow's Nurses, Today - Wolters KluwerMa Mayla Imelda LapaÎncă nu există evaluări
- Best Practices in Simulation PlannDocument11 paginiBest Practices in Simulation Plannraguchandra7527Încă nu există evaluări
- Texto 3 RDocument9 paginiTexto 3 ROmid Ernesto Chahuaris ChoqueÎncă nu există evaluări
- Scalese2008 Article SimulationTechnologyForSkillsTDocument4 paginiScalese2008 Article SimulationTechnologyForSkillsTAbc DefÎncă nu există evaluări
- Ebsco Fulltext 2023 09 22Document9 paginiEbsco Fulltext 2023 09 22api-688059491Încă nu există evaluări
- Elearning Implementation Guide - ENG PDFDocument32 paginiElearning Implementation Guide - ENG PDFcharlesjameskatuaÎncă nu există evaluări
- Teaching Consistent Hand Hygiene: How Can We Improve?: ReviewsDocument8 paginiTeaching Consistent Hand Hygiene: How Can We Improve?: Reviewsvanessa patayonÎncă nu există evaluări
- Development of An E-Learning Module For Clinicians: Case Study: NHS Ayrshire and ArranDocument4 paginiDevelopment of An E-Learning Module For Clinicians: Case Study: NHS Ayrshire and ArranEka AhmadÎncă nu există evaluări
- Activity 1Document3 paginiActivity 1Richelle Mea B. PeñaÎncă nu există evaluări
- Uso de Tecnología para Mantener La Educación de Los Residentes Durante La Pandemia de COVID-19Document4 paginiUso de Tecnología para Mantener La Educación de Los Residentes Durante La Pandemia de COVID-19Yhonni Zela SancaÎncă nu există evaluări
- SimulationDocument9 paginiSimulationKaren Joyce Costales MagtanongÎncă nu există evaluări
- Effects of Simulation-Based Education On Communication Skill and Clinical Competence in Maternity Nursing PracticumDocument9 paginiEffects of Simulation-Based Education On Communication Skill and Clinical Competence in Maternity Nursing PracticumDama Trisa UtamiÎncă nu există evaluări
- Simulation in Nursing: A Constructivist Situated LearningDocument14 paginiSimulation in Nursing: A Constructivist Situated Learningapi-297446309Încă nu există evaluări
- CRM 1Document11 paginiCRM 1nihalhabtiche135Încă nu există evaluări
- Assignment On Clinical Teaching MethodsDocument13 paginiAssignment On Clinical Teaching MethodsSuman Mondal80% (5)
- Teaching and Learning at The BedsideDocument23 paginiTeaching and Learning at The BedsideJohn SummertonÎncă nu există evaluări
- Computer Assisted InstructionDocument4 paginiComputer Assisted InstructionChuche Marie TumarongÎncă nu există evaluări
- Simulation and Its Role in Medical Education: Contemporary IssueDocument6 paginiSimulation and Its Role in Medical Education: Contemporary IssueYorim Sora PasilaÎncă nu există evaluări
- By Charles Larew, Sherrie Lessans, Debra Spunt, Dawn Foster, Barbara CovingtonDocument5 paginiBy Charles Larew, Sherrie Lessans, Debra Spunt, Dawn Foster, Barbara CovingtonAi RimandoÎncă nu există evaluări
- Teaching Clinical Reasoning: A New Playbook: Covid-19 InsightsDocument4 paginiTeaching Clinical Reasoning: A New Playbook: Covid-19 InsightsMahmoud AbouelsoudÎncă nu există evaluări
- PPM Ps 1 12 Patient Centered CareDocument3 paginiPPM Ps 1 12 Patient Centered Careapi-348841675Încă nu există evaluări
- Interaction Between Nurse Anesthetists and Patients in A Highly Technological EnvironmentDocument11 paginiInteraction Between Nurse Anesthetists and Patients in A Highly Technological Environmentapi-348841675Încă nu există evaluări
- Nurse AnesthesiaDocument3 paginiNurse Anesthesiaapi-348841675Încă nu există evaluări
- Past Present FutureDocument9 paginiPast Present Futureapi-348841675Încă nu există evaluări
- (Routledge Anthropology Handbooks) Lenore Manderson (Editor), Elizabeth Cartwright (Editor), Anita Hardon (Editor) - The Routledge Handbook of Medical Anthropology-Routledge (2016)Document424 pagini(Routledge Anthropology Handbooks) Lenore Manderson (Editor), Elizabeth Cartwright (Editor), Anita Hardon (Editor) - The Routledge Handbook of Medical Anthropology-Routledge (2016)Phuong HaÎncă nu există evaluări
- Rape Epidemic in India - Woman and Criminal Law Project ReportDocument12 paginiRape Epidemic in India - Woman and Criminal Law Project ReportNimisha SajekarÎncă nu există evaluări
- Family Environment and Parent Child Relationships As Related To Executive Functioning in ChildrenDocument15 paginiFamily Environment and Parent Child Relationships As Related To Executive Functioning in ChildrenAmy MartínezÎncă nu există evaluări
- Makalah Elektro Terapi (Tens)Document11 paginiMakalah Elektro Terapi (Tens)Filwa FitrianiÎncă nu există evaluări
- Drug Distribution To Human Tissues - Prediction and Examination of The Basic Assumption in in Vivo Pharmacokinetics-Pharmacodynamics ResearchDocument9 paginiDrug Distribution To Human Tissues - Prediction and Examination of The Basic Assumption in in Vivo Pharmacokinetics-Pharmacodynamics Researchopata edward kwameÎncă nu există evaluări
- Standards Guidelines Tools and Techniques Joa Eng 0120Document1 paginăStandards Guidelines Tools and Techniques Joa Eng 0120Kevin Apaza CachacaÎncă nu există evaluări
- Feature WritingDocument3 paginiFeature WritingaddreenaÎncă nu există evaluări
- Formulation and Evaluation of Aceclofenac LiposomeDocument9 paginiFormulation and Evaluation of Aceclofenac LiposomeNikita jainÎncă nu există evaluări
- CPT 1 Questions (50 QNS)Document9 paginiCPT 1 Questions (50 QNS)Unni UnniÎncă nu există evaluări
- Final Socio-Economic Feasibilty Study ReportDocument16 paginiFinal Socio-Economic Feasibilty Study ReportYousuf IÎncă nu există evaluări
- Pork Slaughter HACCP Plan: Rosenthal Meat Science and Technology CenterDocument26 paginiPork Slaughter HACCP Plan: Rosenthal Meat Science and Technology CenterМария УрсуÎncă nu există evaluări
- NGT Feeding: by Group 2Document25 paginiNGT Feeding: by Group 2karl montano100% (1)
- Agar EdwardsDocument2 paginiAgar EdwardsGeraldine CacaceÎncă nu există evaluări
- Part - A (40 Marks) : CLASS X (2020-21) English (Code 0184) Sample Paper-07Document11 paginiPart - A (40 Marks) : CLASS X (2020-21) English (Code 0184) Sample Paper-07krish oswalÎncă nu există evaluări
- FSDS Resources SDN - BHDDocument12 paginiFSDS Resources SDN - BHDRoslyna khanÎncă nu există evaluări
- Why Scorebuilders PTDocument3 paginiWhy Scorebuilders PTSamarÎncă nu există evaluări
- A Protocol For DyingDocument12 paginiA Protocol For DyinggaborkÎncă nu există evaluări
- Making Sense of Media Making Frames of A StoryDocument16 paginiMaking Sense of Media Making Frames of A StoryMike BalubarÎncă nu există evaluări
- Amity Park Walkthrough Version 0.7.3 2Document36 paginiAmity Park Walkthrough Version 0.7.3 2Sayak SahaÎncă nu există evaluări
- Position Sttement CTFA - Skin Lightening - Jan 2022Document1 paginăPosition Sttement CTFA - Skin Lightening - Jan 2022Leila DouganÎncă nu există evaluări
- 2018 ENNS Facts and FiguresDocument360 pagini2018 ENNS Facts and Figuresim.ramÎncă nu există evaluări
- DHA Part B Renal DialysisDocument28 paginiDHA Part B Renal DialysisKiran MauryaÎncă nu există evaluări
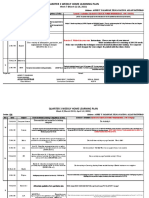
- Week 7 (March 22-26, 2021)Document2 paginiWeek 7 (March 22-26, 2021)Achievers IntelligencesÎncă nu există evaluări
- Occlusal Onlay As Mordern RX PDFDocument13 paginiOcclusal Onlay As Mordern RX PDFSMART SMARÎncă nu există evaluări
- State of Pallaka v. Michael (Defendants)Document33 paginiState of Pallaka v. Michael (Defendants)Kavita73% (11)
- MARIPOSA Soc Sci 3 EssayDocument2 paginiMARIPOSA Soc Sci 3 EssayMichelle MariposaÎncă nu există evaluări
- My CoursesDocument35 paginiMy CoursesSethupathy Lee100% (1)
- Instructions For 2017-18 MBBS Admissons at KIMS KoppalDocument20 paginiInstructions For 2017-18 MBBS Admissons at KIMS KoppalkalloliÎncă nu există evaluări
- Libro Pie WagnerDocument1.390 paginiLibro Pie WagnerarmandoÎncă nu există evaluări
- Propaedeutics of intеrnаl medicine as аn introduction to the clinic of internal medicine. Questioning and physical examination of the patient. Еthical and deontological aspectsDocument42 paginiPropaedeutics of intеrnаl medicine as аn introduction to the clinic of internal medicine. Questioning and physical examination of the patient. Еthical and deontological aspectsDonia HnainiaÎncă nu există evaluări
- Summary: 12 Months to $1 Million: How to Pick a Winning Product, Build a Real Business, and Become a Seven-Figure Entrepreneur by Ryan Daniel Moran: Key Takeaways, Summary & AnalysisDe la EverandSummary: 12 Months to $1 Million: How to Pick a Winning Product, Build a Real Business, and Become a Seven-Figure Entrepreneur by Ryan Daniel Moran: Key Takeaways, Summary & AnalysisEvaluare: 5 din 5 stele5/5 (2)
- The First 90 Days: Proven Strategies for Getting Up to Speed Faster and SmarterDe la EverandThe First 90 Days: Proven Strategies for Getting Up to Speed Faster and SmarterEvaluare: 4.5 din 5 stele4.5/5 (122)
- The 7 Habits of Highly Effective People: The Infographics EditionDe la EverandThe 7 Habits of Highly Effective People: The Infographics EditionEvaluare: 4 din 5 stele4/5 (2475)
- Designing Your Life by Bill Burnett, Dave Evans - Book Summary: How to Build a Well-Lived, Joyful LifeDe la EverandDesigning Your Life by Bill Burnett, Dave Evans - Book Summary: How to Build a Well-Lived, Joyful LifeEvaluare: 4.5 din 5 stele4.5/5 (62)
- Steal the Show: From Speeches to Job Interviews to Deal-Closing Pitches, How to Guarantee a Standing Ovation for All the Performances in Your LifeDe la EverandSteal the Show: From Speeches to Job Interviews to Deal-Closing Pitches, How to Guarantee a Standing Ovation for All the Performances in Your LifeEvaluare: 4.5 din 5 stele4.5/5 (39)
- The Proximity Principle: The Proven Strategy That Will Lead to the Career You LoveDe la EverandThe Proximity Principle: The Proven Strategy That Will Lead to the Career You LoveEvaluare: 4.5 din 5 stele4.5/5 (93)
- The 30 Day MBA: Your Fast Track Guide to Business SuccessDe la EverandThe 30 Day MBA: Your Fast Track Guide to Business SuccessEvaluare: 4.5 din 5 stele4.5/5 (19)
- The 2-Hour Job Search: Using Technology to Get the Right Job FasterDe la EverandThe 2-Hour Job Search: Using Technology to Get the Right Job FasterEvaluare: 4 din 5 stele4/5 (23)
- Ultralearning: Master Hard Skills, Outsmart the Competition, and Accelerate Your CareerDe la EverandUltralearning: Master Hard Skills, Outsmart the Competition, and Accelerate Your CareerEvaluare: 4.5 din 5 stele4.5/5 (361)
- Work Stronger: Habits for More Energy, Less Stress, and Higher Performance at WorkDe la EverandWork Stronger: Habits for More Energy, Less Stress, and Higher Performance at WorkEvaluare: 4.5 din 5 stele4.5/5 (12)
- From Paycheck to Purpose: The Clear Path to Doing Work You LoveDe la EverandFrom Paycheck to Purpose: The Clear Path to Doing Work You LoveEvaluare: 4.5 din 5 stele4.5/5 (39)
- The Everything Guide To Being A Paralegal: Winning Secrets to a Successful Career!De la EverandThe Everything Guide To Being A Paralegal: Winning Secrets to a Successful Career!Evaluare: 5 din 5 stele5/5 (1)
- Start.: Punch Fear in the Face, Escape Average, and Do Work That MattersDe la EverandStart.: Punch Fear in the Face, Escape Average, and Do Work That MattersEvaluare: 4.5 din 5 stele4.5/5 (56)
- The 12 Week Year: Get More Done in 12 Weeks than Others Do in 12 MonthsDe la EverandThe 12 Week Year: Get More Done in 12 Weeks than Others Do in 12 MonthsEvaluare: 4.5 din 5 stele4.5/5 (90)
- Start a Business for Less Than $2,000: From Airbrush Artist to Wellness Instructor, 75+ Profitable Business Startups for Under $2,000De la EverandStart a Business for Less Than $2,000: From Airbrush Artist to Wellness Instructor, 75+ Profitable Business Startups for Under $2,000Evaluare: 5 din 5 stele5/5 (1)
- Job Interview: The Complete Job Interview Preparation and 70 Tough Job Interview Questions with Winning AnswersDe la EverandJob Interview: The Complete Job Interview Preparation and 70 Tough Job Interview Questions with Winning AnswersEvaluare: 4 din 5 stele4/5 (7)
- 12 Habits Of Valuable Employees: Your Roadmap to an Amazing CareerDe la Everand12 Habits Of Valuable Employees: Your Roadmap to an Amazing CareerÎncă nu există evaluări
- The Ultimate Side Hustle Book: 450 Moneymaking Ideas for the Gig EconomyDe la EverandThe Ultimate Side Hustle Book: 450 Moneymaking Ideas for the Gig EconomyEvaluare: 4 din 5 stele4/5 (1)
- The Resume and Cover Letter Phrase Book: What to Write to Get the Job That's RightDe la EverandThe Resume and Cover Letter Phrase Book: What to Write to Get the Job That's RightEvaluare: 4 din 5 stele4/5 (9)
- The Dictionary of Body Language: A Field Guide to Human BehaviorDe la EverandThe Dictionary of Body Language: A Field Guide to Human BehaviorEvaluare: 4.5 din 5 stele4.5/5 (96)
- What Every BODY is Saying: An Ex-FBI Agent’s Guide to Speed-Reading PeopleDe la EverandWhat Every BODY is Saying: An Ex-FBI Agent’s Guide to Speed-Reading PeopleEvaluare: 4.5 din 5 stele4.5/5 (354)
- Motivated Mindset: Kick Procrastination to the CurbDe la EverandMotivated Mindset: Kick Procrastination to the CurbEvaluare: 4.5 din 5 stele4.5/5 (43)
- The Unspoken Rules: Secrets to Starting Your Career Off RightDe la EverandThe Unspoken Rules: Secrets to Starting Your Career Off RightEvaluare: 5 din 5 stele5/5 (7)