S-ar putea să vă placă și
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Your Consequences WorksheetDocument10 paginiYour Consequences WorksheetThe Center for Motivation and ChangeÎncă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Acupuncture, Trigger Points and Musculoskeletal Pain - Peter E. BaldryDocument378 paginiAcupuncture, Trigger Points and Musculoskeletal Pain - Peter E. Baldrygerkenp100% (6)
- Blood Cells and Its Types With FunctionsDocument5 paginiBlood Cells and Its Types With Functionskaleb16_2Încă nu există evaluări
- Motorcycle DiariesDocument9 paginiMotorcycle DiariesGelo De Guzman100% (1)
- Sexually Transmitted InfectionsDocument110 paginiSexually Transmitted Infectionstummalapalli venkateswara raoÎncă nu există evaluări
- Basic EpidemiologyDocument257 paginiBasic EpidemiologydhanaÎncă nu există evaluări
- Analytical Method Validation of Clopidogrel Tablets BR HPLCDocument48 paginiAnalytical Method Validation of Clopidogrel Tablets BR HPLCAman ThakurÎncă nu există evaluări
- R 41 TH KLLDocument20 paginiR 41 TH KLLmiraÎncă nu există evaluări
- R 41 TH KLLDocument20 paginiR 41 TH KLLmiraÎncă nu există evaluări
- R 41 TH KLLDocument20 paginiR 41 TH KLLmiraÎncă nu există evaluări
- R 41 TH KLLDocument20 paginiR 41 TH KLLmiraÎncă nu există evaluări
- Af 22 TH KLLDocument20 paginiAf 22 TH KLLMaidilla SilviaÎncă nu există evaluări
- Ger 1Document8 paginiGer 1miraÎncă nu există evaluări
- Grand Rounds: Jinghua Chen, MD, PHD July 15Th, 2016Document23 paginiGrand Rounds: Jinghua Chen, MD, PHD July 15Th, 2016miraÎncă nu există evaluări
- Af 22 TH KLLDocument20 paginiAf 22 TH KLLMaidilla SilviaÎncă nu există evaluări
- Total Mechanical Bowel Obs MekongDocument16 paginiTotal Mechanical Bowel Obs MekongmiraÎncă nu există evaluări
- Gambar SkillabDocument1 paginăGambar SkillabmiraÎncă nu există evaluări
- Daftar PustakaDocument1 paginăDaftar PustakamiraÎncă nu există evaluări
- L 42 TH Diffuse Peritonitis DT Hollow Organ PerforationDocument16 paginiL 42 TH Diffuse Peritonitis DT Hollow Organ PerforationmiraÎncă nu există evaluări
- Pneumothorax MekongDocument14 paginiPneumothorax MekongmiraÎncă nu există evaluări
- Vital Signs: Temperature: Respiratory Rate: PulseDocument55 paginiVital Signs: Temperature: Respiratory Rate: PulsemiraÎncă nu există evaluări
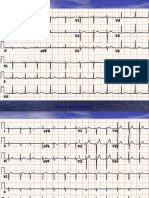
- Gambar ECGDocument40 paginiGambar ECGmiraÎncă nu există evaluări
- ECG Praktis DR HanantoDocument43 paginiECG Praktis DR HanantomiraÎncă nu există evaluări
- DR Wong Teck WeeipadDocument2 paginiDR Wong Teck Weeipadtwwong68Încă nu există evaluări
- Medical Guidelines 2014-15Document453 paginiMedical Guidelines 2014-15soleiman.ariaÎncă nu există evaluări
- Fycompa Efficacy Adjunctive Partial SeizuresDocument20 paginiFycompa Efficacy Adjunctive Partial SeizuresoneniravÎncă nu există evaluări
- Giant Skin TagDocument2 paginiGiant Skin Tagshf.mxlikÎncă nu există evaluări
- Evaluation of scales in immune-mediated polyneuropathiesDocument222 paginiEvaluation of scales in immune-mediated polyneuropathiesAngelo MalerbaÎncă nu există evaluări
- Elgabri v. Lekas, M.D., 1st Cir. (1992)Document21 paginiElgabri v. Lekas, M.D., 1st Cir. (1992)Scribd Government DocsÎncă nu există evaluări
- The LungsDocument6 paginiThe LungsnandaÎncă nu există evaluări
- Class 11 English Snapshots Chapter 7Document2 paginiClass 11 English Snapshots Chapter 7Alpha StarÎncă nu există evaluări
- Introduction to Radiographic Imaging InterpretationDocument17 paginiIntroduction to Radiographic Imaging Interpretationpradep4u21Încă nu există evaluări
- Influence of The Quality of The FinishedDocument6 paginiInfluence of The Quality of The Finishedmehdi chahrourÎncă nu există evaluări
- Essential and Non-Essential Fatty Acids PDFDocument4 paginiEssential and Non-Essential Fatty Acids PDFBj Delacruz100% (2)
- Science Blood TransfusionsDocument10 paginiScience Blood Transfusionsapi-237866019Încă nu există evaluări
- Resume 2019Document1 paginăResume 2019api-316723361Încă nu există evaluări
- Colgate Oral Care: Product RangeDocument62 paginiColgate Oral Care: Product RangeRahuls RahulsÎncă nu există evaluări
- EFN - PPTX 3Document9 paginiEFN - PPTX 3Suheni Khotimah IndrianiÎncă nu există evaluări
- This Just In!: Queen Pin Carla!Document10 paginiThis Just In!: Queen Pin Carla!BS Central, Inc. "The Buzz"Încă nu există evaluări
- Drug Study - VancomycinDocument2 paginiDrug Study - VancomycinKhatlen BagaresÎncă nu există evaluări
- Case Study of Mrs. WalkerDocument4 paginiCase Study of Mrs. WalkerPreet ChahalÎncă nu există evaluări
- MGR Medical University Medal WinnersDocument17 paginiMGR Medical University Medal WinnersElavarasanÎncă nu există evaluări
- Masterlist SummaryDocument6 paginiMasterlist Summarykentclark03Încă nu există evaluări
- Dissertation Topics 2Document21 paginiDissertation Topics 2Apollo Institute of Hospital Administration100% (1)
- Spironolactone Class Indications: 25MG TAB, 50Mg Tab, 100Mg TabDocument2 paginiSpironolactone Class Indications: 25MG TAB, 50Mg Tab, 100Mg TabAhmad KusayiriÎncă nu există evaluări
- The Divine Message of Yog Rishi.: Swastha Ho Jan, Gan, Man and The Nation 'Document68 paginiThe Divine Message of Yog Rishi.: Swastha Ho Jan, Gan, Man and The Nation 'Aniket ShahÎncă nu există evaluări