S-ar putea să vă placă și
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Epidemiologic ApproachDocument38 paginiThe Epidemiologic ApproachGlaneisia MitchellÎncă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Faringitis StreptococcusDocument16 paginiFaringitis StreptococcusnurÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Antiepileptic Drugs ThesisDocument5 paginiAntiepileptic Drugs Thesisfjf8xxz4100% (2)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- 8-Ecg in CovidsDocument35 pagini8-Ecg in CovidsyandraÎncă nu există evaluări
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- 19.sinonasal TumorsDocument246 pagini19.sinonasal Tumorsfabian hernandez medinaÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Bronchial ObstructionDocument137 paginiBronchial ObstructionGrajdianu Natalia100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Subcutaneous MycosesDocument22 paginiSubcutaneous MycosesCut Raihan100% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Definition of Kidney StonesDocument4 paginiDefinition of Kidney StonesArul MÎncă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Manual Handling Case Studies Part 1 - Attempt Review PDFDocument30 paginiManual Handling Case Studies Part 1 - Attempt Review PDFMODI KRUNAL100% (2)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- CefuroximeDocument11 paginiCefuroximeAlmira Ballesteros CestonaÎncă nu există evaluări
- Paranoid Personality Disorder: Case ReportDocument3 paginiParanoid Personality Disorder: Case ReporttTTÎncă nu există evaluări
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Increased Intracranial Pressure (IICP)Document2 paginiIncreased Intracranial Pressure (IICP)Giselle Chloe Baluya icoÎncă nu există evaluări
- Management of Medically Compromised PatientsDocument70 paginiManagement of Medically Compromised PatientsPriyanka WadhawanÎncă nu există evaluări
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Pituitary Disorders - Adrenal Disorders - Thyroid DiseasesDocument207 paginiPituitary Disorders - Adrenal Disorders - Thyroid Diseasesnurliah armandÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- 4.BST GIM Post Summary Form - DermatologyDocument3 pagini4.BST GIM Post Summary Form - Dermatologyjosiah masukaÎncă nu există evaluări
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- ATLS Examination Questions and Answers 2019Document4 paginiATLS Examination Questions and Answers 2019Kamalan Push25% (8)
- 28-2016-04-022 - DR Farhan Ahmed MajeedDocument5 pagini28-2016-04-022 - DR Farhan Ahmed MajeedAndika Budi Kusuma PutraÎncă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- MRCS Practice Papers Part A: Paper 2 Emqs: Second EditionDocument28 paginiMRCS Practice Papers Part A: Paper 2 Emqs: Second Editionhina arsh0% (1)
- Care Plan Prep May 13 Rheumatic FeverDocument16 paginiCare Plan Prep May 13 Rheumatic Feverapi-256360167Încă nu există evaluări
- SbarDocument2 paginiSbarbojums100% (2)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Meniere's DiseaseDocument2 paginiMeniere's DiseaseNoelyn BaluyanÎncă nu există evaluări
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
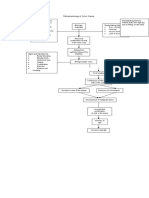
- Pathophysiology of Colon Cancer Predisposing Factors: Etiology: Precipitating Factors: Precipitating FactorsDocument1 paginăPathophysiology of Colon Cancer Predisposing Factors: Etiology: Precipitating Factors: Precipitating FactorstatiÎncă nu există evaluări
- Breast Cancer Awareness - 13 October 2019Document4 paginiBreast Cancer Awareness - 13 October 2019Times MediaÎncă nu există evaluări
- Adji Suranto. Khasiat Dan Manfaat Madu Herbal (Jakarta: Agromedia Pustaka, 2004)Document2 paginiAdji Suranto. Khasiat Dan Manfaat Madu Herbal (Jakarta: Agromedia Pustaka, 2004)Dania Shafa AlmasaÎncă nu există evaluări
- Bhopal (M.P.) : Case Presentation On Bipolar-ManicDocument19 paginiBhopal (M.P.) : Case Presentation On Bipolar-ManicamitÎncă nu există evaluări
- GRTP Wallet Card FinalDocument2 paginiGRTP Wallet Card FinalIrish FroggyÎncă nu există evaluări
- Distribution and Density of Tertiary Lymphoid Structures Predict Clinical Outcome in Intrahepatic CholangiocarcinomaDocument12 paginiDistribution and Density of Tertiary Lymphoid Structures Predict Clinical Outcome in Intrahepatic Cholangiocarcinoma马三强Încă nu există evaluări
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- 04 Taking A Case HistoryDocument38 pagini04 Taking A Case HistoryMwanja MosesÎncă nu există evaluări
- Literature Feeding and Eating Quick GuideDocument17 paginiLiterature Feeding and Eating Quick GuideHana alassafÎncă nu există evaluări
- A Child Is Gasping For Breath But Has A Pulse Rate of 100 Per MinuteDocument2 paginiA Child Is Gasping For Breath But Has A Pulse Rate of 100 Per Minuteferri100% (1)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)