S-ar putea să vă placă și
- Kelompok 3 - Naskah Role Play Timbang TerimaDocument7 paginiKelompok 3 - Naskah Role Play Timbang TerimaFerdy Bayu SaputraÎncă nu există evaluări
- 321efektivitas Bayam Dan Buah Bit Terhadap Kadar Hemoglobin Ibu HamilDocument12 pagini321efektivitas Bayam Dan Buah Bit Terhadap Kadar Hemoglobin Ibu Hamilsindy marveniaÎncă nu există evaluări
- Leaflet MPKPDocument2 paginiLeaflet MPKPSubi YantoÎncă nu există evaluări
- Nyeri Post SCDocument32 paginiNyeri Post SCFrntzn LrnÎncă nu există evaluări
- Advanced History TakingDocument15 paginiAdvanced History TakingErik DewantoÎncă nu există evaluări
- LP Speech DelayDocument16 paginiLP Speech DelayLina LinaNaÎncă nu există evaluări
- Format JurnalDocument16 paginiFormat JurnalRetno puspitariniÎncă nu există evaluări
- Lembar Pengajuan Judul SkripsiDocument4 paginiLembar Pengajuan Judul SkripsiAnggi Rizky Adhi PratamaÎncă nu există evaluări
- RM 13 (Checklist Harian Discharge Planning)Document2 paginiRM 13 (Checklist Harian Discharge Planning)nurisÎncă nu există evaluări
- Asuhan Kebidanan Pra Nikah Dan Pra Konsepsi Program Profesi BidanDocument7 paginiAsuhan Kebidanan Pra Nikah Dan Pra Konsepsi Program Profesi BidanKopi Senja BaturradenÎncă nu există evaluări
- Peran Orang Tua Dengan Kemandirian Personal Hygiene Pada Anak Prasekolah Usia 3Document6 paginiPeran Orang Tua Dengan Kemandirian Personal Hygiene Pada Anak Prasekolah Usia 3Yon Yon100% (1)
- JBI - Ceklist Cross Sectional 1Document9 paginiJBI - Ceklist Cross Sectional 1Nabilah Mukti RifahmiÎncă nu există evaluări
- MANUSKRIPDocument11 paginiMANUSKRIPandika saputraÎncă nu există evaluări
- Fix Makalah EnglishDocument25 paginiFix Makalah EnglishkezyaaaaaÎncă nu există evaluări
- Perawatan Diri Ibu Primipara Selama Periode Nifas (Revisi)Document24 paginiPerawatan Diri Ibu Primipara Selama Periode Nifas (Revisi)FerdilaDilaAmandaÎncă nu există evaluări
- Brosur UnipduDocument6 paginiBrosur UnipduNuning ArmawatiÎncă nu există evaluări
- Dukungan Suami DGN Kemauan AsiDocument7 paginiDukungan Suami DGN Kemauan AsiMariaÎncă nu există evaluări
- ANALISIS JURNAL PICO & VRA AYI SUMIATIDocument17 paginiANALISIS JURNAL PICO & VRA AYI SUMIATIputraÎncă nu există evaluări
- Makalah RW SiagaDocument11 paginiMakalah RW SiagaUli Rahma Dini SÎncă nu există evaluări
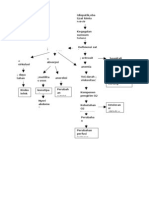
- Pathway AnemiaDocument1 paginăPathway AnemiaRayn ChristÎncă nu există evaluări
- Log Book Kangaroo Mother CareDocument3 paginiLog Book Kangaroo Mother CareYan BaseriÎncă nu există evaluări
- Analisa Kasus HIPERGLIKEMIDocument30 paginiAnalisa Kasus HIPERGLIKEMIanis dwi prakasiwiÎncă nu există evaluări
- Biokimia KankerDocument105 paginiBiokimia KankerErics EfranyÎncă nu există evaluări
- 26 19 1 SM PDFDocument8 pagini26 19 1 SM PDFAndika Nofriawan SaputraÎncă nu există evaluări
- AbcDocument7 paginiAbcLingga NurhayatiÎncă nu există evaluări
- MANUSCRIP - Diah Oktaviani PDFDocument10 paginiMANUSCRIP - Diah Oktaviani PDFIqvi Arnida AyuningtyasÎncă nu există evaluări
- Sabrina Salsabila-Fkik PDFDocument178 paginiSabrina Salsabila-Fkik PDFHersan RÎncă nu există evaluări
- Bhasa InggrisDocument23 paginiBhasa InggrisrinaÎncă nu există evaluări
- Pathway SCDocument2 paginiPathway SCRizky TiaraÎncă nu există evaluări
- Promkes PPDocument56 paginiPromkes PPwisnuÎncă nu există evaluări
- Lta FiveDocument100 paginiLta FiveEchy RahmadhaniÎncă nu există evaluări
- Askep Sirosis HatiDocument48 paginiAskep Sirosis HatiWidya AryantiÎncă nu există evaluări
- Bhs InggrisDocument16 paginiBhs InggrisMuhammad WardiÎncă nu există evaluări
- Meisi Arisandi - Resume Jurnal Internasional Dan Nasional Keperawatan JiwaDocument4 paginiMeisi Arisandi - Resume Jurnal Internasional Dan Nasional Keperawatan JiwawendihiÎncă nu există evaluări
- Bahan NurseprenuerDocument4 paginiBahan NurseprenuerNova Triska Purnama SariÎncă nu există evaluări
- Temperamen Dan Praktik Pengasuhan Orang Tua Menentukan Perkembangan Sosial Emosi Anak Usia PrasekolahDocument20 paginiTemperamen Dan Praktik Pengasuhan Orang Tua Menentukan Perkembangan Sosial Emosi Anak Usia PrasekolahAulia SyalwaaÎncă nu există evaluări
- Pathways AidsDocument1 paginăPathways AidsSayhidoen CepexÎncă nu există evaluări
- Lembar ObsDocument4 paginiLembar ObsYan BaseriÎncă nu există evaluări
- Sumber Artikel 1Document17 paginiSumber Artikel 1Lili ApriliaÎncă nu există evaluări
- Self Efficacy Ibu Hamil Trimester Iii: Dengan Tingkat Kecemasan Dalam Menghadapi PersalinanDocument10 paginiSelf Efficacy Ibu Hamil Trimester Iii: Dengan Tingkat Kecemasan Dalam Menghadapi PersalinanZeviÎncă nu există evaluări
- CswsDocument3 paginiCswsratnadwsÎncă nu există evaluări
- 274 25 PBDocument63 pagini274 25 PBPutri Utami HadiyatiÎncă nu există evaluări
- Brosur Klinik VCTDocument2 paginiBrosur Klinik VCTNila WatiÎncă nu există evaluări
- Pengaruh Pemberian Aromaterapi Jahe Terh 2Document7 paginiPengaruh Pemberian Aromaterapi Jahe Terh 2Lastri Khairin100% (1)
- Nilai Normal TTVDocument32 paginiNilai Normal TTVNyemas syakmiÎncă nu există evaluări
- LP&SPTK RPK (Nadia Nur Alfu P27905119020)Document18 paginiLP&SPTK RPK (Nadia Nur Alfu P27905119020)nadia nur AlfuÎncă nu există evaluări
- Askep Bahasa InggrisDocument7 paginiAskep Bahasa InggrisPuputÎncă nu există evaluări
- Askep Pada Anak Dengan GNA, GNC, NS PDFDocument17 paginiAskep Pada Anak Dengan GNA, GNC, NS PDFIndah MilleniaÎncă nu există evaluări
- Percakapan Bahasa InggrisDocument6 paginiPercakapan Bahasa InggrisCaeyu Sche CuahyaÎncă nu există evaluări
- Pengaruh Prenatal Gentle Yoga Dalam Menurunkan Tingkat Kecemasan Pada Ibu Hamil Trimester IIIDocument7 paginiPengaruh Prenatal Gentle Yoga Dalam Menurunkan Tingkat Kecemasan Pada Ibu Hamil Trimester IIIp17331174047 YUNIFA ANWARÎncă nu există evaluări
- 102 196 1 SMDocument7 pagini102 196 1 SMlaminar sibaraniÎncă nu există evaluări
- IHC PPT TemplateDocument25 paginiIHC PPT TemplateNely SilviaÎncă nu există evaluări
- LP WahamDocument17 paginiLP WahamBlue HeartÎncă nu există evaluări
- Soal Aggregate Community NursingDocument11 paginiSoal Aggregate Community NursingAde Ima NovikasariÎncă nu există evaluări
- JURNAL Alifka OkDocument8 paginiJURNAL Alifka OkAlifka PratiwiÎncă nu există evaluări
- Diagram Layang Analisa Swot Ruang Krissan Rsud BangilDocument2 paginiDiagram Layang Analisa Swot Ruang Krissan Rsud BangilDacxa GrohamÎncă nu există evaluări
- Euro J of Neurology - 2023 - Kincl - Parkinson S Disease Cardiovascular Symptoms A New Complex Functional and StructuralDocument9 paginiEuro J of Neurology - 2023 - Kincl - Parkinson S Disease Cardiovascular Symptoms A New Complex Functional and StructuralIvan MihailovicÎncă nu există evaluări
- ADHF ManagementDocument6 paginiADHF ManagementEsti YunitaÎncă nu există evaluări
- Fsurg 09 851113Document7 paginiFsurg 09 851113Cuide e se CuideÎncă nu există evaluări
- DIAB10.1002@ccd.28194 4Document9 paginiDIAB10.1002@ccd.28194 4marsim92Încă nu există evaluări
- The Science of Sleep: A Brief Guide On How To Sleep Better Every NightDocument2 paginiThe Science of Sleep: A Brief Guide On How To Sleep Better Every NightMark Anthony RaymundoÎncă nu există evaluări
- Atlas of Nerve Conduction Studies and Electromyography (2 Ed.)Document21 paginiAtlas of Nerve Conduction Studies and Electromyography (2 Ed.)rodrigocorcino899959Încă nu există evaluări
- Sr. No. Cghs Treatment Procedure/Investigation List Non-NABH/Non - NABL Rates Nabh/Nabl RatesDocument49 paginiSr. No. Cghs Treatment Procedure/Investigation List Non-NABH/Non - NABL Rates Nabh/Nabl RatesADDECC INFO INDIAÎncă nu există evaluări
- Embryonic Stem CellsDocument6 paginiEmbryonic Stem CellsTakwa ShlakiÎncă nu există evaluări
- DSGT MCQ 3Document3 paginiDSGT MCQ 3Anil KaleÎncă nu există evaluări
- Botox Consent Form EnglishDocument2 paginiBotox Consent Form Englishargha mandrawataÎncă nu există evaluări
- Sally Aburumman Bushra SaleemDocument75 paginiSally Aburumman Bushra SaleemAbdulrahman AlsayyedÎncă nu există evaluări
- Bearing Habits and Garden Practices To Induce FruitfulnessDocument6 paginiBearing Habits and Garden Practices To Induce FruitfulnessHEGDErv1964Încă nu există evaluări
- Oxoid 2012-13Document84 paginiOxoid 2012-13Athar AbbasÎncă nu există evaluări
- Cardiac Rehabilitation.Document60 paginiCardiac Rehabilitation.Salman KhanÎncă nu există evaluări
- Applications of Biological Anthropology To Human Affairs - C. G. Nicholas Mascie-... (2005, PDFDocument263 paginiApplications of Biological Anthropology To Human Affairs - C. G. Nicholas Mascie-... (2005, PDFkenÎncă nu există evaluări
- Set A: Community Health Nursing and Care of Mother and ChildDocument11 paginiSet A: Community Health Nursing and Care of Mother and ChildAldrin NavarroÎncă nu există evaluări
- Life Expectancy Powerpoint PresentationDocument6 paginiLife Expectancy Powerpoint PresentationAlejandro MendozaÎncă nu există evaluări
- Test Bank For College Algebra 12Th Edition by Lial Hornsby Schneider and Daniels Isbn 0134217454 978013421745 Full Chapter PDFDocument36 paginiTest Bank For College Algebra 12Th Edition by Lial Hornsby Schneider and Daniels Isbn 0134217454 978013421745 Full Chapter PDFdavid.weldon592100% (12)
- Annex A - Self-Assessment Tool For Proposed EPCB Health Facilities PDFDocument5 paginiAnnex A - Self-Assessment Tool For Proposed EPCB Health Facilities PDFCora Mendoza100% (1)
- Nursing Process of PneumoniaDocument5 paginiNursing Process of Pneumoniatin2x061275% (8)
- Pathophysiology and Management of Diabetes Mellitus GppqeDocument60 paginiPathophysiology and Management of Diabetes Mellitus GppqeOlivia OliverÎncă nu există evaluări
- 1) Introduction To Microbiology - HistoryDocument37 pagini1) Introduction To Microbiology - HistoryJustin Dave ManantanÎncă nu există evaluări
- Clinical Chemistry Notes With BlanksDocument34 paginiClinical Chemistry Notes With Blanksepson printerÎncă nu există evaluări
- Speaking Part 3 Update 2022Document7 paginiSpeaking Part 3 Update 2022Nhi LêÎncă nu există evaluări
- Atrial Fibrillation - Diagnosis and Treatment - AAFP PDFDocument8 paginiAtrial Fibrillation - Diagnosis and Treatment - AAFP PDFNaufal AmanullahÎncă nu există evaluări
- Drug StudyDocument4 paginiDrug StudySharwen_R_Rome_5572Încă nu există evaluări
- OsteoarthritisDocument4 paginiOsteoarthritisDharti PatelÎncă nu există evaluări
- Does WiFi Affect The BrainDocument6 paginiDoes WiFi Affect The BrainrustyÎncă nu există evaluări
- Failure of Endoscopic Spine SurgeryDocument6 paginiFailure of Endoscopic Spine SurgeryKaustubh KeskarÎncă nu există evaluări
- III Bds II Internal 2023Document5 paginiIII Bds II Internal 2023Sourab KumarÎncă nu există evaluări
- KOICA Application FormDocument12 paginiKOICA Application Formdeni100% (1)
- Pyle Et Al 1995 - Rapid Direct Count E ColiDocument7 paginiPyle Et Al 1995 - Rapid Direct Count E ColiFabio SenaÎncă nu există evaluări
- Slide Jurnal Reading 2Document20 paginiSlide Jurnal Reading 2WulanSyafitriÎncă nu există evaluări
- 2021-05-15 New ScientistDocument62 pagini2021-05-15 New ScientistAgenor Phillips100% (1)