S-ar putea să vă placă și
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Bid ProcessDocument85 paginiBid ProcessRobiatol Adawiah Mohammad ShamsidiÎncă nu există evaluări
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- MF 5460Document586 paginiMF 5460Maximiliano Hitschfeld100% (2)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Properties of Skeletal MuscleDocument72 paginiProperties of Skeletal MuscleAakash GohilÎncă nu există evaluări
- Bashar Discusses Monatomics, White Powder Gold and Ormus MineralsDocument32 paginiBashar Discusses Monatomics, White Powder Gold and Ormus MineralsFlorin V. Iagaru100% (6)
- Collection of Books To Read Preparing For ACM ICPCDocument1 paginăCollection of Books To Read Preparing For ACM ICPCJia Hong100% (2)
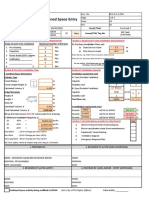
- Ventilation Plan For Confined Space EntryDocument9 paginiVentilation Plan For Confined Space EntryMohamad Nazmi Mohamad Rafian100% (1)
- RAN KPI MonitorDocument8 paginiRAN KPI MonitorOmer WaqarÎncă nu există evaluări
- HypnosisDocument2 paginiHypnosisEsteban MendozaÎncă nu există evaluări
- AGITAN Defoamer Technologies PDFDocument15 paginiAGITAN Defoamer Technologies PDFMarco Lopez100% (1)
- The Housekeeping Department: Learning Activity #1Document4 paginiThe Housekeeping Department: Learning Activity #1Limar Geoff G. RosalesÎncă nu există evaluări
- 20752-Reservoir Management Training An Lntegrated ApproachDocument6 pagini20752-Reservoir Management Training An Lntegrated ApproachdanonninoÎncă nu există evaluări
- Stepper Motor Interface Board: Application ManualDocument43 paginiStepper Motor Interface Board: Application ManualMohamed Ismail100% (1)
- Tuomo Summanen Michael Pollitt: Case Study: British Telecom: Searching For A Winning StrategyDocument34 paginiTuomo Summanen Michael Pollitt: Case Study: British Telecom: Searching For A Winning StrategyRanganath ChowdaryÎncă nu există evaluări
- Usg Sheetrock® Brand Acoustical SealantDocument3 paginiUsg Sheetrock® Brand Acoustical SealantHoracio PadillaÎncă nu există evaluări
- Appendix 1c Bridge Profiles Allan TrussesDocument43 paginiAppendix 1c Bridge Profiles Allan TrussesJosue LewandowskiÎncă nu există evaluări
- Middle Range TheoriesDocument134 paginiMiddle Range TheoriesMary Joyce MejiaÎncă nu există evaluări
- Anagrams in Enhancing The Learner's Vocabolary in Filipino Language Using WordwallDocument19 paginiAnagrams in Enhancing The Learner's Vocabolary in Filipino Language Using WordwallJARYL PILLAZARÎncă nu există evaluări
- Research 3Document30 paginiResearch 3Lorenzo Maxwell GarciaÎncă nu există evaluări
- Vehicle and Driver Vibration - PPTDocument16 paginiVehicle and Driver Vibration - PPTAnirban MitraÎncă nu există evaluări
- Safety and Arming Device Timer 6-7-1976Document5 paginiSafety and Arming Device Timer 6-7-1976nguyenhÎncă nu există evaluări
- Reynaers Product Overview CURTAIN WALLDocument80 paginiReynaers Product Overview CURTAIN WALLyantoÎncă nu există evaluări
- TDS VH202 Steel Spore Discs B - Atrophaeus Cell Line 9372 SDN 06 Rev. 1.0Document3 paginiTDS VH202 Steel Spore Discs B - Atrophaeus Cell Line 9372 SDN 06 Rev. 1.0Muhammad FirdausÎncă nu există evaluări
- General Psychology Module 1.1Document6 paginiGeneral Psychology Module 1.1Niño Gabriel MagnoÎncă nu există evaluări
- "Smart Attendance Using F Ttendance Management Using Face Recognition" Anagement SystemDocument13 pagini"Smart Attendance Using F Ttendance Management Using Face Recognition" Anagement Systemamer HÎncă nu există evaluări
- Research Associate in The DFG Graduate Program - Collective Decision-Making - (12 Positions) - 28 Subsection 3 HMBHGDocument3 paginiResearch Associate in The DFG Graduate Program - Collective Decision-Making - (12 Positions) - 28 Subsection 3 HMBHGFiya ShahÎncă nu există evaluări
- SANY HDForklift Brochure-112018Document14 paginiSANY HDForklift Brochure-112018Rossman Mejicanos100% (1)
- KTO12 Curriculum ExplainedDocument24 paginiKTO12 Curriculum ExplainedErnesto ViilavertÎncă nu există evaluări
- Vision and Mission Analysis ChapterDocument15 paginiVision and Mission Analysis Chapterzaza bazazaÎncă nu există evaluări
- Curios AllianceDocument32 paginiCurios AllianceyesterowÎncă nu există evaluări
- CSC309 Extra Credit 1Document5 paginiCSC309 Extra Credit 1Fluffy BagelzÎncă nu există evaluări