S-ar putea să vă placă și
- The Duty for Sponor Oversight in Clinical Trials: Practical Guide: 2nd Edition Clinical Data ReviewDe la EverandThe Duty for Sponor Oversight in Clinical Trials: Practical Guide: 2nd Edition Clinical Data ReviewÎncă nu există evaluări
- Clinical Research ExplainedDocument27 paginiClinical Research ExplainedupendernathiÎncă nu există evaluări
- GSK b2c109575 Clinical Study Report Redact PDFDocument1.524 paginiGSK b2c109575 Clinical Study Report Redact PDFdhananjayÎncă nu există evaluări
- Site FDA inspection checklistDocument9 paginiSite FDA inspection checklistsreeraj.guruvayoorÎncă nu există evaluări
- The Practical Guide to Clinical Research and PublicationDe la EverandThe Practical Guide to Clinical Research and PublicationÎncă nu există evaluări
- Research Protocol TemplateDocument6 paginiResearch Protocol TemplateAshref BelhajÎncă nu există evaluări
- 06 PSUR PBRER Thomas MunzDocument35 pagini06 PSUR PBRER Thomas MunzMohabKamalÎncă nu există evaluări
- Investigators Responsibilities With GCPDocument16 paginiInvestigators Responsibilities With GCPLlosa JuneÎncă nu există evaluări
- Clinical Guidelines Ecbs 2001Document52 paginiClinical Guidelines Ecbs 2001Ajay KumarÎncă nu există evaluări
- GCP protects human subjects in clinical researchDocument3 paginiGCP protects human subjects in clinical researchSok YeeÎncă nu există evaluări
- CTD Modules PDFDocument5 paginiCTD Modules PDFsrideviÎncă nu există evaluări
- SITE GEN-001 01 - SOP On Site ActivitiesDocument17 paginiSITE GEN-001 01 - SOP On Site ActivitiesCR Professionals IndiaÎncă nu există evaluări
- Developing and Writing CRFDocument23 paginiDeveloping and Writing CRFsuri333Încă nu există evaluări
- Ethical Issues in Clinical ResearchDocument33 paginiEthical Issues in Clinical ResearchSenthil ThyagarajanÎncă nu există evaluări
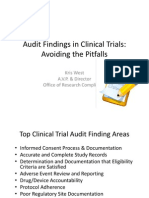
- Audit Findings in Clinical TrialsDocument21 paginiAudit Findings in Clinical TrialsMohit SinghÎncă nu există evaluări
- The Study Protocol Part TwoDocument12 paginiThe Study Protocol Part TwoGerman LambogliaÎncă nu există evaluări
- Clinical Trial DocumentsDocument37 paginiClinical Trial Documentsapi-37446750% (1)
- Ich GCPDocument4 paginiIch GCPRaju GundaramÎncă nu există evaluări
- Clinical Trial ChecklistDocument3 paginiClinical Trial ChecklistIzzi FekratÎncă nu există evaluări
- Guidelines Phase1 Clinical TrialsDocument64 paginiGuidelines Phase1 Clinical TrialsJinnatÎncă nu există evaluări
- Clinical Trial Transparency (TranspariMED 2017) 20171212Document40 paginiClinical Trial Transparency (TranspariMED 2017) 20171212Till BrucknerÎncă nu există evaluări
- Fundamentals of Biologicals Regulation: Vaccines and Biotechnology MedicinesDe la EverandFundamentals of Biologicals Regulation: Vaccines and Biotechnology MedicinesEvaluare: 5 din 5 stele5/5 (1)
- Key Concepts of Clinical Trials A Narrative ReviewDocument12 paginiKey Concepts of Clinical Trials A Narrative ReviewLaura CampañaÎncă nu există evaluări
- Essential Elements of Clinical TrialDocument39 paginiEssential Elements of Clinical TrialmisganaÎncă nu există evaluări
- An Introduction To Clinical Trials (Jonathan A. Cook)Document277 paginiAn Introduction To Clinical Trials (Jonathan A. Cook)Nitin AnitaÎncă nu există evaluări
- Protocol Template - Early Phase.2Document36 paginiProtocol Template - Early Phase.2Vasiliy KÎncă nu există evaluări
- Clinical Trial DesignsDocument18 paginiClinical Trial DesignsVenkatesh Gavini100% (1)
- Clinical Research OrganizationDocument2 paginiClinical Research OrganizationnehacodeslabÎncă nu există evaluări
- Cra GuideDocument17 paginiCra Guidebitterlemon01Încă nu există evaluări
- Essentail Documents For Conduct of A Clinical TrialDocument26 paginiEssentail Documents For Conduct of A Clinical TrialFarah Aman KhanÎncă nu există evaluări
- Seefeld-Statistics Using R With Biological Examples PDFDocument325 paginiSeefeld-Statistics Using R With Biological Examples PDFManuel LoGaÎncă nu există evaluări
- Downtown Hotel Feasibility StudyDocument84 paginiDowntown Hotel Feasibility StudyMohammad Ahmad Ayasrah100% (2)
- Using Realworld Data For Outcomes Research and Comparative Effectiveness StudiesDocument44 paginiUsing Realworld Data For Outcomes Research and Comparative Effectiveness StudiesTest Download100% (1)
- Nonclinical Safety Assessment: A Guide to International Pharmaceutical RegulationsDe la EverandNonclinical Safety Assessment: A Guide to International Pharmaceutical RegulationsWilliam J. BrockÎncă nu există evaluări
- 05 Ich GCPDocument25 pagini05 Ich GCPBhaskar Satya Sankar Balaji100% (1)
- Protocol Designing in CTDocument5 paginiProtocol Designing in CTSushma Reddy VÎncă nu există evaluări
- Human Research Protection Program Informed Consent ProcessDocument6 paginiHuman Research Protection Program Informed Consent ProcessNurul KurniawatiÎncă nu există evaluări
- 10 - Drug DevelopmentDocument5 pagini10 - Drug DevelopmentLaura SaglietiÎncă nu există evaluări
- DateDocument5 paginiDatehazshuuÎncă nu există evaluări
- Clinical Trials Data ManagementDocument3 paginiClinical Trials Data ManagementAyush JainÎncă nu există evaluări
- CLN-20 00 Investigational Product HandlingDocument4 paginiCLN-20 00 Investigational Product Handlingpopatlilo2Încă nu există evaluări
- A Clinical Study ReportDocument57 paginiA Clinical Study ReportAbhi RamÎncă nu există evaluări
- Retrospective Protocol TemplateDocument6 paginiRetrospective Protocol TemplateSymonJosef ConchaÎncă nu există evaluări
- Ich-Gcp & Schedule yDocument38 paginiIch-Gcp & Schedule ySahiti PendyalaÎncă nu există evaluări
- Discrepancy ManagementDocument34 paginiDiscrepancy Managementnikunj_patel_4367% (6)
- Handbook of Intelligent Scaffolds For Tissue Engineering and Regenerative MedicineDocument32 paginiHandbook of Intelligent Scaffolds For Tissue Engineering and Regenerative Medicineaalizadeh_325% (4)
- Documentation of Clinical Trial Monitoring: A practical guide compliant with Good Clinical PracticeDe la EverandDocumentation of Clinical Trial Monitoring: A practical guide compliant with Good Clinical PracticeEvaluare: 5 din 5 stele5/5 (1)
- Ethical Considerations When Preparing a Clinical Research ProtocolDe la EverandEthical Considerations When Preparing a Clinical Research ProtocolÎncă nu există evaluări
- Clinical Research ClassDocument110 paginiClinical Research ClassEreshÎncă nu există evaluări
- 2 Topical Fluoride For Caries Prevention 2013 UpdateDocument118 pagini2 Topical Fluoride For Caries Prevention 2013 UpdateHub SciÎncă nu există evaluări
- RAPS Online U CatalogDocument22 paginiRAPS Online U CatalogvinayÎncă nu există evaluări
- Protocol Template 05feb2016 508Document3 paginiProtocol Template 05feb2016 508Dwi Annisa AmaliaSariÎncă nu există evaluări
- Schedule YDocument30 paginiSchedule Yapi-3810976100% (13)
- Sop Title: Assessing Protocol Feasibility: Sop No: Effective DateDocument7 paginiSop Title: Assessing Protocol Feasibility: Sop No: Effective Datetiara rengganis100% (1)
- Clinical Research OverviewDocument40 paginiClinical Research Overviewjyoti100% (1)
- Clinical Research AssociateDocument2 paginiClinical Research AssociatepalkybdÎncă nu există evaluări
- EVALUATING CLINICAL Studies of Antimicrobials in The Division of Antiinfective Drug ProductsDocument102 paginiEVALUATING CLINICAL Studies of Antimicrobials in The Division of Antiinfective Drug ProductsMichael wang100% (1)
- Ind Studies by Sejal KhumanDocument34 paginiInd Studies by Sejal KhumanSejal khumamÎncă nu există evaluări
- RUSSIAN DRUG REGISTRATION CHANGESDocument9 paginiRUSSIAN DRUG REGISTRATION CHANGESashwanÎncă nu există evaluări
- Automated Signal DetectionDocument7 paginiAutomated Signal DetectionSutirtho MukherjiÎncă nu există evaluări
- FDA Guidance PMS and Clinical TrialsDocument21 paginiFDA Guidance PMS and Clinical TrialsJonna SapiterÎncă nu există evaluări
- Works For Sanofi AventisDocument6 paginiWorks For Sanofi AventisMohit AroraÎncă nu există evaluări
- FDA drug development overviewDocument1 paginăFDA drug development overviewsapis18Încă nu există evaluări
- Clinical Study ReportDocument5 paginiClinical Study ReportAlexandraCirlanÎncă nu există evaluări
- A Practical Guide On Pharmacovigilance For BeginnersDocument10 paginiA Practical Guide On Pharmacovigilance For Beginnerssreeraj.guruvayoorÎncă nu există evaluări
- Clinical Study Report: Prevalence of Peripheral Arterial Disease in Acute Coronary Syndrome PatientsDocument4 paginiClinical Study Report: Prevalence of Peripheral Arterial Disease in Acute Coronary Syndrome PatientsRadu AnaÎncă nu există evaluări
- Clinical Biochemistry & Analytical ToxicologyDocument4 paginiClinical Biochemistry & Analytical ToxicologyRohit Manakchand ZawarÎncă nu există evaluări
- BASIC PHARMACOKINETICS-Ch2: Mathematics ReviewDocument75 paginiBASIC PHARMACOKINETICS-Ch2: Mathematics ReviewDrHeba100% (5)
- Clinical Study Advertising Clinical StudiesDocument1 paginăClinical Study Advertising Clinical StudiesRohit Manakchand ZawarÎncă nu există evaluări
- Tdr/Tdp/Sop/99 1Document36 paginiTdr/Tdp/Sop/99 1abhiyanaÎncă nu există evaluări
- ICMR Ethical Guidelines (India)Document77 paginiICMR Ethical Guidelines (India)api-3836189100% (2)
- STI Operational GuidelinesDocument152 paginiSTI Operational GuidelineskishorechandraÎncă nu există evaluări
- Cognitive-Behavioral Therapy For Adult Anxiety Disorders in Clinical Practice: A Meta-Analysis of Effectiveness StudiesDocument13 paginiCognitive-Behavioral Therapy For Adult Anxiety Disorders in Clinical Practice: A Meta-Analysis of Effectiveness StudiesMaria Inês de AzevedoÎncă nu există evaluări
- ARDS Meduri JAMA 1998Document8 paginiARDS Meduri JAMA 1998Rivaneide AmorimÎncă nu există evaluări
- What We Need From You: Please Return Page 2 Via Fax To (512) 738-8397Document2 paginiWhat We Need From You: Please Return Page 2 Via Fax To (512) 738-8397Tàrár ŁàráibÎncă nu există evaluări
- Antenatal Education and Postnatal Support Strategies PDFDocument7 paginiAntenatal Education and Postnatal Support Strategies PDFNoraÎncă nu există evaluări
- High Blood Pressure in Acute Ischaemic Stroke - Broadening Therapeutic HorizonsDocument7 paginiHigh Blood Pressure in Acute Ischaemic Stroke - Broadening Therapeutic HorizonsSergio Gutierrez VidalÎncă nu există evaluări
- IBS DiareDocument12 paginiIBS Diarejokeshua34Încă nu există evaluări
- Do School Bags Cause Back Pain?Document6 paginiDo School Bags Cause Back Pain?TÎncă nu există evaluări
- OTCtxDocument3 paginiOTCtxlosangelesÎncă nu există evaluări
- Lesson 2 - Univariate Statistics and Experimental DesignDocument34 paginiLesson 2 - Univariate Statistics and Experimental Designsteven231191Încă nu există evaluări
- Fingolimoid - 2014Document9 paginiFingolimoid - 2014rodicasept1967Încă nu există evaluări
- Placebo EffectDocument3 paginiPlacebo EffectsmarterÎncă nu există evaluări
- PreskripsiDocument80 paginiPreskripsiIdfy BagusÎncă nu există evaluări
- Sept NewsletterDocument12 paginiSept NewsletterLouiseÎncă nu există evaluări
- CROs in BelgiumDocument7 paginiCROs in BelgiumAna ConstantinescuÎncă nu există evaluări
- 2007, Vol.25, Issues 1, Photodynamic TherapyDocument114 pagini2007, Vol.25, Issues 1, Photodynamic TherapyRizweta DestinÎncă nu există evaluări
- NICE Guidelines For Dental RecallDocument24 paginiNICE Guidelines For Dental Recallnaomi0% (1)
- Atropine Treatment 1Document7 paginiAtropine Treatment 1Chris ChowÎncă nu există evaluări
- Luc Montagnier, Nobel Prize Winner, Takes Homeopathy SeriouslyDocument8 paginiLuc Montagnier, Nobel Prize Winner, Takes Homeopathy SeriouslypathiayoÎncă nu există evaluări
- A Day in The Life of A Medical DirectorDocument21 paginiA Day in The Life of A Medical DirectorMuhammad AbeeshÎncă nu există evaluări
- Broad-spectrum antibiotics for preterm prelabor rupture of fetal membranesDocument10 paginiBroad-spectrum antibiotics for preterm prelabor rupture of fetal membranesmaxis4xÎncă nu există evaluări
- 1B-Prevalence of Hearing LossDocument2 pagini1B-Prevalence of Hearing LossNafisa ZamanÎncă nu există evaluări
- 33Document23 pagini33salaminiaÎncă nu există evaluări