S-ar putea să vă placă și
- Psychiatry Practice BoostersDe la EverandPsychiatry Practice BoostersJesse KoskeyÎncă nu există evaluări
- Somatoform and Other Psychosomatic Disorders: A Dialogue Between Contemporary Psychodynamic Psychotherapy and Cognitive Behavioral Therapy PerspectivesDe la EverandSomatoform and Other Psychosomatic Disorders: A Dialogue Between Contemporary Psychodynamic Psychotherapy and Cognitive Behavioral Therapy PerspectivesChristos CharisÎncă nu există evaluări
- Positive and Negative Syndrome Scale (PANSS) Training: Challenges, SolutionsDocument5 paginiPositive and Negative Syndrome Scale (PANSS) Training: Challenges, SolutionsZachÎncă nu există evaluări
- Rating Scales for Assessing Bipolar Disorder SymptomsDocument14 paginiRating Scales for Assessing Bipolar Disorder SymptomsDivia RainaÎncă nu există evaluări
- Terms in The Field of Psychiatry and NeurologyDocument25 paginiTerms in The Field of Psychiatry and NeurologyMarlon SigfredÎncă nu există evaluări
- Case Presentation PBL 12 Bipolar DisorderDocument65 paginiCase Presentation PBL 12 Bipolar DisorderKim S GutierrezÎncă nu există evaluări
- Module 3 Biochemistry of The BrainDocument12 paginiModule 3 Biochemistry of The BrainSakshi Jauhari100% (1)
- Schizophrenia: Causes, Incidence, and Risk FactorsDocument3 paginiSchizophrenia: Causes, Incidence, and Risk FactorsNurul Hidayah IbrahimÎncă nu există evaluări
- Mobile Clinic Mobile PSE GuideDocument18 paginiMobile Clinic Mobile PSE GuideFrancisco Javier Salazar Núñez100% (1)
- Wells Brief Cognitive Therapy For Social Phobia - A Case SeriesDocument8 paginiWells Brief Cognitive Therapy For Social Phobia - A Case SeriesjuaromerÎncă nu există evaluări
- Bernard Gallagher Cap. 5 Sociology of Mental IllnessDocument16 paginiBernard Gallagher Cap. 5 Sociology of Mental IllnessLaura CristinaÎncă nu există evaluări
- Prodromal SchizophreniaDocument13 paginiProdromal SchizophreniadizhalfaÎncă nu există evaluări
- Relationship Between Premorbid Functioning and Symptom Severity As Assessed at First Episode of PsychosisDocument6 paginiRelationship Between Premorbid Functioning and Symptom Severity As Assessed at First Episode of Psychosisaldrin19Încă nu există evaluări
- Physical and Mental Disability TestDocument9 paginiPhysical and Mental Disability TestANITTA SÎncă nu există evaluări
- Mood DisordersDocument6 paginiMood Disordersapi-217446206Încă nu există evaluări
- A Case Study of A Mental DisorderDocument7 paginiA Case Study of A Mental DisorderMaurine TuitoekÎncă nu există evaluări
- Psychiatry Notes - Defenses MechanismsDocument2 paginiPsychiatry Notes - Defenses MechanismsLiSenÎncă nu există evaluări
- Individual Music Therapy For Depression: Randomised Controlled TrialDocument9 paginiIndividual Music Therapy For Depression: Randomised Controlled TrialSarah HarahapÎncă nu există evaluări
- Cognitive Function in Schizophrenia A Review 187 PDFDocument8 paginiCognitive Function in Schizophrenia A Review 187 PDFEvaÎncă nu există evaluări
- Final ThesisDocument120 paginiFinal ThesisSingh SoniyaÎncă nu există evaluări
- 21.cpsy.034 Icd-10&dsm-5Document8 pagini21.cpsy.034 Icd-10&dsm-5Victor YanafÎncă nu există evaluări
- Case Analysis Assignment: Interpersonal and Social Rhythm TherapyDocument2 paginiCase Analysis Assignment: Interpersonal and Social Rhythm TherapyJoshua RingorÎncă nu există evaluări
- Assessment & Management of Dissociative Disorders: Chairperson: DR - Safeekh A.T. Presenter: Dr.D.ArchanaaDocument62 paginiAssessment & Management of Dissociative Disorders: Chairperson: DR - Safeekh A.T. Presenter: Dr.D.Archanaadrkadiyala2Încă nu există evaluări
- Negative Symptoms EQZ Lancet ReviewDocument14 paginiNegative Symptoms EQZ Lancet ReviewConstanza González GutiérrezÎncă nu există evaluări
- Psych Case StudyDocument14 paginiPsych Case StudySmridhi Seth100% (1)
- The Columbia Suicide Severity Rating Scale PDFDocument21 paginiThe Columbia Suicide Severity Rating Scale PDFTri Anny Rakhmawati0% (1)
- Common Psychiatric TermsDocument6 paginiCommon Psychiatric TermsKatrina Heart Rauto AvilaÎncă nu există evaluări
- The Clinical Assessment Interview For Negative SymDocument9 paginiThe Clinical Assessment Interview For Negative SymJohanes DavidÎncă nu există evaluări
- CDI Patient VersionDocument9 paginiCDI Patient VersionalotfyaÎncă nu există evaluări
- What Is SchizophreniaDocument6 paginiWhat Is SchizophreniaSeLeCtAh RiCkYÎncă nu există evaluări
- Understanding Schizophrenia: Symptoms, Causes and TreatmentDocument31 paginiUnderstanding Schizophrenia: Symptoms, Causes and Treatmentmed studentÎncă nu există evaluări
- Psychiatry: ' ' Psychology 538 ' Pathology 540 ' Pharmacology 556Document24 paginiPsychiatry: ' ' Psychology 538 ' Pathology 540 ' Pharmacology 556Brush LowdryÎncă nu există evaluări
- General Questions (Mood Disorder)Document5 paginiGeneral Questions (Mood Disorder)Zubair MushtaqÎncă nu există evaluări
- Coexistence of Folie Communique e and Folie SimultaneeDocument4 paginiCoexistence of Folie Communique e and Folie SimultaneeAna Rosa González Barroso0% (1)
- SchizophreniaDocument2 paginiSchizophreniaIT’S ME HAYLA100% (1)
- Intro Child PsychiatryDocument122 paginiIntro Child PsychiatryayunisallehÎncă nu există evaluări
- An Update On The Comorbidity of ADHD and ASDDocument16 paginiAn Update On The Comorbidity of ADHD and ASDCristina SolerÎncă nu există evaluări
- Borderline Personality DisorderDocument6 paginiBorderline Personality DisorderPersephona13Încă nu există evaluări
- 1999 Aversion Therapy-BEDocument6 pagini1999 Aversion Therapy-BEprabhaÎncă nu există evaluări
- Assisted Outpatient Treatment in New York State: The Case For Making Kendra's Law PermanentDocument16 paginiAssisted Outpatient Treatment in New York State: The Case For Making Kendra's Law PermanentManhattan InstituteÎncă nu există evaluări
- PsychiatryDocument23 paginiPsychiatryNaveenKumarÎncă nu există evaluări
- Psychiatry Capstone 43020 Agitation PsychopharmacologyDocument20 paginiPsychiatry Capstone 43020 Agitation Psychopharmacologyapi-552282470Încă nu există evaluări
- Geriatric Psychiatry LectureDocument113 paginiGeriatric Psychiatry LectureabrihamÎncă nu există evaluări
- Psychiatry and Aging - A Powerpoint PresentationDocument55 paginiPsychiatry and Aging - A Powerpoint PresentationShivan A.C.0% (2)
- InsomniaDocument313 paginiInsomniaRaudhah FadhilahÎncă nu există evaluări
- Assessment ToolsDocument74 paginiAssessment ToolsSharvari ShahÎncă nu există evaluări
- Physical Examination Skills Vital for PsychiatristsDocument8 paginiPhysical Examination Skills Vital for PsychiatristsDita Mega UtamiÎncă nu există evaluări
- Hess BenoitWritingHistoryPsychiatryDocument8 paginiHess BenoitWritingHistoryPsychiatryIvo VarlaÎncă nu există evaluări
- H.5.1 Antipsychotics PowerPoint 2016Document55 paginiH.5.1 Antipsychotics PowerPoint 2016Ptrc Lbr LpÎncă nu există evaluări
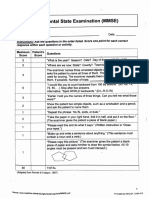
- Mini-Mental State Examination (MMSE)Document3 paginiMini-Mental State Examination (MMSE)Prescilla San PedroÎncă nu există evaluări
- Neuroanatomy For The Psychiatrist: Textbook of PsychiatryDocument37 paginiNeuroanatomy For The Psychiatrist: Textbook of Psychiatrykrysdana22Încă nu există evaluări
- CEP BPSD Discussion Guide ENG RFCG Updated2019 PDFDocument8 paginiCEP BPSD Discussion Guide ENG RFCG Updated2019 PDFM.DalaniÎncă nu există evaluări
- Role of Vitamin D in Schizophrenia in Elderly PatientDocument3 paginiRole of Vitamin D in Schizophrenia in Elderly PatientJAVED ATHER SIDDIQUIÎncă nu există evaluări
- Case Analysis: Bipolar 1 Diagnosis & Treatment PlanDocument2 paginiCase Analysis: Bipolar 1 Diagnosis & Treatment PlanJoshua Ringor100% (1)
- Mental Health Information For Children: Child PsychiatryDocument9 paginiMental Health Information For Children: Child Psychiatryedawood2100% (2)
- Brain Imaging in PsychiatryDocument7 paginiBrain Imaging in PsychiatryKaram Ali ShahÎncă nu există evaluări
- Notes On PsychiatryDocument10 paginiNotes On PsychiatryMark VillenaÎncă nu există evaluări
- Code of Conduct (IACP-1995) : To StrengthenDocument39 paginiCode of Conduct (IACP-1995) : To StrengthenklockÎncă nu există evaluări
- Psychiatry Case LogDocument6 paginiPsychiatry Case Logf3er3Încă nu există evaluări
- Schizoaffective Disorder FactsheetDocument6 paginiSchizoaffective Disorder FactsheetYusnida RahmawatiÎncă nu există evaluări
- De-Regil Et Al-2016-The Cochrane LibraryDocument124 paginiDe-Regil Et Al-2016-The Cochrane LibrarytriaclaresiaÎncă nu există evaluări
- Flunarizine Effective Migrainous Vertigo PreventionDocument6 paginiFlunarizine Effective Migrainous Vertigo PreventionNanda WtÎncă nu există evaluări
- A Comparative Effectiveness Meta-Analysis of Drugs For The Prophylaxis of Migraine HeadacheDocument60 paginiA Comparative Effectiveness Meta-Analysis of Drugs For The Prophylaxis of Migraine HeadachetriaclaresiaÎncă nu există evaluări
- Oxygen For Cluster Headaches: A GuideDocument25 paginiOxygen For Cluster Headaches: A GuidetriaclaresiaÎncă nu există evaluări
- Tugas Ekspertise AbdomenDocument42 paginiTugas Ekspertise AbdomentriaclaresiaÎncă nu există evaluări
- E. HystoliticaDocument7 paginiE. HystoliticatriaclaresiaÎncă nu există evaluări
- Creamer Et Al-2016-British Journal of DermatologyDocument34 paginiCreamer Et Al-2016-British Journal of DermatologyAtika Indah SariÎncă nu există evaluări
- Supplementation of Vitamin D in Pregnancy and Its Correlation With Feto-Maternal OutcomeDocument20 paginiSupplementation of Vitamin D in Pregnancy and Its Correlation With Feto-Maternal OutcometriaclaresiaÎncă nu există evaluări
- Initial Severity of Schizophrenia and EfficacyDocument20 paginiInitial Severity of Schizophrenia and EfficacytriaclaresiaÎncă nu există evaluări
- Benign Paroxysmal Positional VertigoDocument65 paginiBenign Paroxysmal Positional VertigoReni SusantiÎncă nu există evaluări
- Perioperative Dextromethorphan As An Adjunct For Postoperative PainDocument10 paginiPerioperative Dextromethorphan As An Adjunct For Postoperative PaintriaclaresiaÎncă nu există evaluări
- Yoi 140088Document779 paginiYoi 140088triaclaresiaÎncă nu există evaluări
- Guidelines For The Administration of Blood and Blood ComponentsDocument29 paginiGuidelines For The Administration of Blood and Blood ComponentsCindya PerthyÎncă nu există evaluări
- Clinical Use of BloodDocument221 paginiClinical Use of BloodRizma Adlia100% (1)
- MeniereDocument50 paginiMenieretriaclaresiaÎncă nu există evaluări
- BPPVDocument36 paginiBPPVRizka AmaliaÎncă nu există evaluări
- Introduction To Serology - Immunology, HSV & H.pyloriDocument37 paginiIntroduction To Serology - Immunology, HSV & H.pyloritriaclaresiaÎncă nu există evaluări
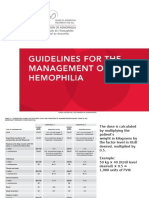
- Dosis HemofiliaDocument5 paginiDosis HemofiliatriaclaresiaÎncă nu există evaluări
- S1 Diet, Immune and InfectionDocument48 paginiS1 Diet, Immune and InfectiontriaclaresiaÎncă nu există evaluări
- MUPIROCINDocument2 paginiMUPIROCINNathalie kate petallarÎncă nu există evaluări
- DKADocument64 paginiDKAAravindhan Gunasekaran PaediatricianÎncă nu există evaluări
- Contoh CV Profesi Farmasi Dalam Bahasa InggriaDocument1 paginăContoh CV Profesi Farmasi Dalam Bahasa InggriaGita Namiramasri100% (2)
- Hospital Case Study FlexsimDocument2 paginiHospital Case Study FlexsimMano KanthanathanÎncă nu există evaluări
- HW 1 PathoDocument4 paginiHW 1 PathoBryan RallomaÎncă nu există evaluări
- Rogers 2017Document29 paginiRogers 2017UmerÎncă nu există evaluări
- Managing corticosteroids and their side effectsDocument6 paginiManaging corticosteroids and their side effectsKrista Madranca CastroÎncă nu există evaluări
- Subacute, Silent, and Postpartum Thyroiditis 2012Document11 paginiSubacute, Silent, and Postpartum Thyroiditis 2012YoaNnita GoMezÎncă nu există evaluări
- Contoh Presentasi JurnalDocument13 paginiContoh Presentasi JurnalElisha Rosalyn0% (1)
- Testing Anxiety in Undergraduate Medical Students and Its Correlation With Different Learning ApproachesDocument11 paginiTesting Anxiety in Undergraduate Medical Students and Its Correlation With Different Learning ApproachesJosé Carlos Sánchez-RamirezÎncă nu există evaluări
- Alcohol Binge Drinking in OCDDocument2 paginiAlcohol Binge Drinking in OCDSuyash DwivediÎncă nu există evaluări
- Diaz 2009Document1 paginăDiaz 2009Nasrudin EfendiÎncă nu există evaluări
- Learning Objective: - Explain of Acute AbdomenDocument143 paginiLearning Objective: - Explain of Acute AbdomenSamuel Sebastian SirapanjiÎncă nu există evaluări
- Record Keeping A Pocket Guide 005 343Document6 paginiRecord Keeping A Pocket Guide 005 343ryanbucoÎncă nu există evaluări
- Curriculum Vitae - Carla CarnesDocument2 paginiCurriculum Vitae - Carla Carnesccarnes2Încă nu există evaluări
- Managing Hypertension Through Lifestyle ChangesDocument3 paginiManaging Hypertension Through Lifestyle ChangespsychyzeÎncă nu există evaluări
- Poster Template 20201217 10Document1 paginăPoster Template 20201217 10api-538973019Încă nu există evaluări
- Suppurative Lung DIseaseDocument33 paginiSuppurative Lung DIseaseNur Liyana Ahmad ZakiÎncă nu există evaluări
- Kayla Adkins Policy Action Plan Nur 420Document9 paginiKayla Adkins Policy Action Plan Nur 420api-499926602Încă nu există evaluări
- Making Sense of The New Guidelines: Hypertension: The More We Learn, The Less We KnowDocument37 paginiMaking Sense of The New Guidelines: Hypertension: The More We Learn, The Less We KnowMuhammad Nur ArifinÎncă nu există evaluări
- New & Improved Neurological AssessmentDocument39 paginiNew & Improved Neurological AssessmentkixfrondaÎncă nu există evaluări
- Natural Cure CenterDocument7 paginiNatural Cure CenterNandhini ArunÎncă nu există evaluări
- NEUROPrelims - History Taking in NeurologyDocument4 paginiNEUROPrelims - History Taking in NeurologyRenatoCosmeGalvanJuniorÎncă nu există evaluări
- Self LigationDocument2 paginiSelf Ligationdavidrocks81Încă nu există evaluări
- Perinatal AuditDocument11 paginiPerinatal AuditGladys SusantyÎncă nu există evaluări
- Protooncogene Tyrosineprotein Kinase Srcrelated Mouth Pyogenic Granuloma An Investigation Involving 2 InstanceskermbDocument2 paginiProtooncogene Tyrosineprotein Kinase Srcrelated Mouth Pyogenic Granuloma An Investigation Involving 2 Instanceskermbsaucebelief33Încă nu există evaluări
- Psychotherapy TypesDocument36 paginiPsychotherapy TypessilencedurevesÎncă nu există evaluări
- Resume Only 2018Document2 paginiResume Only 2018api-430903191Încă nu există evaluări
- Neonatal SepsisDocument8 paginiNeonatal SepsisPrabiñKhadkaÎncă nu există evaluări
- Echs EmpanelmentDocument316 paginiEchs EmpanelmentYudhvir SawhneyÎncă nu există evaluări