S-ar putea să vă placă și
- Cataract PPT FinalDocument37 paginiCataract PPT FinalSibi John91% (22)
- Sure Success in Ophthalmology Viva Voce & Practical Examination - 2013 PDFDocument300 paginiSure Success in Ophthalmology Viva Voce & Practical Examination - 2013 PDFKaran Kumarswamy79% (14)
- Kuhn 2016Document548 paginiKuhn 2016Karan Kumarswamy100% (1)
- MIRA Scleral Buckling Components 2009Document1 paginăMIRA Scleral Buckling Components 2009Karan KumarswamyÎncă nu există evaluări
- Eye Clinic in Manila City: List of Eye ClinicsDocument12 paginiEye Clinic in Manila City: List of Eye ClinicsJamesBuensalidoDellava100% (1)
- Macular HoleDocument80 paginiMacular HoleRaissaÎncă nu există evaluări
- Eyelids Diseases Lacrimal System DiseasesDocument45 paginiEyelids Diseases Lacrimal System DiseasesMAMA LALAÎncă nu există evaluări
- Pa MataDocument115 paginiPa MataIchsan WidjanarkoÎncă nu există evaluări
- Anatomy of Peripheral RetinaDocument29 paginiAnatomy of Peripheral RetinaNeelam Khatwani100% (1)
- PterygiumDocument40 paginiPterygiumKhurram ChauhanÎncă nu există evaluări
- 6.ANAtomy of CORNEA SrisDocument108 pagini6.ANAtomy of CORNEA SrisSristi ThakurÎncă nu există evaluări
- Glaucoma: Consultant OphthalmologistDocument45 paginiGlaucoma: Consultant OphthalmologistGladys MainaÎncă nu există evaluări
- Ocular Surface Squamous Neoplasia (Ossn)Document59 paginiOcular Surface Squamous Neoplasia (Ossn)nellieauthorÎncă nu există evaluări
- Retinal DetachmentDocument3 paginiRetinal DetachmentzeejayÎncă nu există evaluări
- Dr. Indra DIAGNOSTIC FEATURES IN DIABETIC RETINOPATHYDocument11 paginiDr. Indra DIAGNOSTIC FEATURES IN DIABETIC RETINOPATHYdeprot87Încă nu există evaluări
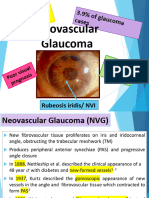
- Rana Greene Neovascular GlaucomaDocument25 paginiRana Greene Neovascular GlaucomaGG IÎncă nu există evaluări
- Tobacco-Alcohol Amblyopia A MaculopathyDocument19 paginiTobacco-Alcohol Amblyopia A MaculopathycarmenÎncă nu există evaluări
- Age-Related Macular DegenerationDocument53 paginiAge-Related Macular DegenerationAbegail IbañezÎncă nu există evaluări
- Eyelid PathologyDocument55 paginiEyelid PathologyleahÎncă nu există evaluări
- Pathology of The: John R. Minarcik, M.DDocument78 paginiPathology of The: John R. Minarcik, M.Drush73Încă nu există evaluări
- Corneal DegenerationDocument1 paginăCorneal Degenerationtgrrwccj98Încă nu există evaluări
- Cataracts: ClassificationDocument9 paginiCataracts: ClassificationRafay ChacharÎncă nu există evaluări
- Choroidal Coloboma: Presenter:Dr. Rahul Moderator: Dr. ArchisDocument48 paginiChoroidal Coloboma: Presenter:Dr. Rahul Moderator: Dr. ArchisjihanÎncă nu există evaluări
- Miopi X Katarak 4Document5 paginiMiopi X Katarak 4Melati Nurul UtamiÎncă nu există evaluări
- Leukocoria: Regan Januardy Marliau I11109020Document28 paginiLeukocoria: Regan Januardy Marliau I11109020Anjar NuryantoÎncă nu există evaluări
- Hereditary Vitreoretinal DegenerationsDocument11 paginiHereditary Vitreoretinal DegenerationsImtiaz AhmedÎncă nu există evaluări
- Pathogenisis of Rhegmatogenous RDDocument23 paginiPathogenisis of Rhegmatogenous RDUsman SadiqÎncă nu există evaluări
- Macular Hole: DR Samarth MishraDocument42 paginiMacular Hole: DR Samarth MishraUliana-Ariadna BozulÎncă nu există evaluări
- Pterygium Ambreen ppt1Document87 paginiPterygium Ambreen ppt1Syeda F AmbreenÎncă nu există evaluări
- KERATOCONUSDocument22 paginiKERATOCONUSAarush DeoraÎncă nu există evaluări
- Diseases of The Eyelids: Mshangila Barnabas MD, M.MedDocument31 paginiDiseases of The Eyelids: Mshangila Barnabas MD, M.MedCharles AnthonyÎncă nu există evaluări
- March 2019 Ophthalmic PearlsDocument2 paginiMarch 2019 Ophthalmic PearlsApps OmÎncă nu există evaluări
- Glaucoma & CataractDocument53 paginiGlaucoma & CataractBenita100% (1)
- Masahito Ohji - Surgical Retina-Springer Singapore (2019)Document115 paginiMasahito Ohji - Surgical Retina-Springer Singapore (2019)María Reneé Jiménez SotomayorÎncă nu există evaluări
- 30secondary GlaucomasDocument19 pagini30secondary GlaucomasShari' Si WahyuÎncă nu există evaluări
- Eye Path12Document45 paginiEye Path12JillKellyÎncă nu există evaluări
- Retina AnswersDocument5 paginiRetina AnswersKhushal Khan KakarÎncă nu există evaluări
- Patologi MataDocument78 paginiPatologi Mataanita awÎncă nu există evaluări
- GLAUKOMADocument47 paginiGLAUKOMARahma GhnÎncă nu există evaluări
- Giant Hanging Melanoma of The Eye SkinDocument2 paginiGiant Hanging Melanoma of The Eye SkinRochnald PigaiÎncă nu există evaluări
- Sympathetic OphthalmiaDocument27 paginiSympathetic OphthalmiaAnish KumarÎncă nu există evaluări
- Retinal Hemangiomas - American Academy of OphthalmologyDocument10 paginiRetinal Hemangiomas - American Academy of OphthalmologyLydia Angelia YanitaÎncă nu există evaluări
- 19 Rationale of Retinal Detachment ManagementDocument87 pagini19 Rationale of Retinal Detachment ManagementvajasaÎncă nu există evaluări
- KeratoconusDocument10 paginiKeratoconusbijujcÎncă nu există evaluări
- Presentation 2Document57 paginiPresentation 2medhanit anjuloÎncă nu există evaluări
- Mata Tenang Visus Turun MendadakDocument34 paginiMata Tenang Visus Turun MendadakTanani 102014007Încă nu există evaluări
- Retinoblastoma 2019Document15 paginiRetinoblastoma 2019lenirizkiÎncă nu există evaluări
- (OPTHA) Lec 5 - RetinaDocument5 pagini(OPTHA) Lec 5 - RetinaPatricia ManaliliÎncă nu există evaluări
- Limbal DermoidDocument4 paginiLimbal DermoidPranjali ChhayaÎncă nu există evaluări
- Glaucoma, Hyphema: Synonyms and Related Keywords: Hyphema, Microhyphema, Hemorrhage in The AnteriorDocument22 paginiGlaucoma, Hyphema: Synonyms and Related Keywords: Hyphema, Microhyphema, Hemorrhage in The AnteriorWulandari EmyÎncă nu există evaluări
- Cornea and ScleraDocument144 paginiCornea and SclerakhabibtopgÎncă nu există evaluări
- Age-Related Macular Disease: Fitriani Umi Hasanah 201820401011121 Pembimbing: Dr. Fatin Hamamah, SP.MDocument28 paginiAge-Related Macular Disease: Fitriani Umi Hasanah 201820401011121 Pembimbing: Dr. Fatin Hamamah, SP.MKim NayoungÎncă nu există evaluări
- April 2017 Ophthalmic PearlsDocument2 paginiApril 2017 Ophthalmic PearlsNur Asri AinunÎncă nu există evaluări
- Pathology of The: John R. Minarcik, M.DDocument78 paginiPathology of The: John R. Minarcik, M.DDEWI MULYANIÎncă nu există evaluări
- Retinal DetachmentDocument21 paginiRetinal Detachmentณัช เกษมÎncă nu există evaluări
- Opthalma Passmedicin 2020Document157 paginiOpthalma Passmedicin 2020VikrantÎncă nu există evaluări
- Lecture Injuries of Organ of Vision.Document47 paginiLecture Injuries of Organ of Vision.rajarajachozhan139Încă nu există evaluări
- Pterigium Dan Pendarahan SubkonjungtivaDocument24 paginiPterigium Dan Pendarahan SubkonjungtivaRasya DanardhonoÎncă nu există evaluări
- Degenerative MyopiaDocument53 paginiDegenerative MyopiaNiloy BasakÎncă nu există evaluări
- Ophthalmology EmergenciesDocument60 paginiOphthalmology Emergenciesasraf amirullahÎncă nu există evaluări
- GLAUCOMADocument7 paginiGLAUCOMAAndrea TamundongÎncă nu există evaluări
- Management of Retinal Detachment: A Guide For Non-OphthalmologistsDocument6 paginiManagement of Retinal Detachment: A Guide For Non-OphthalmologistsadriantiariÎncă nu există evaluări
- Mira Ophth NotesDocument27 paginiMira Ophth NotesMorticia AddamsÎncă nu există evaluări
- Clinical Ophthalmology for Undergraduates by Shahzad WaseemDe la EverandClinical Ophthalmology for Undergraduates by Shahzad WaseemEvaluare: 4 din 5 stele4/5 (5)
- Khata RegistrationDocument5 paginiKhata RegistrationKaran KumarswamyÎncă nu există evaluări
- Zeiss Visulas 532 - Quick GuideDocument2 paginiZeiss Visulas 532 - Quick GuideKaran KumarswamyÎncă nu există evaluări
- Enhanced Depth Imaging Optical Coherence TomographyDocument10 paginiEnhanced Depth Imaging Optical Coherence TomographyKaran KumarswamyÎncă nu există evaluări
- IBEPE StudyDocument8 paginiIBEPE StudyKaran KumarswamyÎncă nu există evaluări
- Collaborative Ocular Melanoma Study (COMS) Findings: Small Medium LargeDocument3 paginiCollaborative Ocular Melanoma Study (COMS) Findings: Small Medium LargeKaran KumarswamyÎncă nu există evaluări
- Target Pressures in Glaucoma: Key WordsDocument5 paginiTarget Pressures in Glaucoma: Key WordsKaran KumarswamyÎncă nu există evaluări
- Melanocytoma of The Optic Nerve Head: Clinical Case - Photo EssayDocument5 paginiMelanocytoma of The Optic Nerve Head: Clinical Case - Photo EssayKaran KumarswamyÎncă nu există evaluări
- Dnausb1007aaa04 WWW 20050425Document2 paginiDnausb1007aaa04 WWW 20050425Karan KumarswamyÎncă nu există evaluări
- Anti - VEGF Agents: Presenter - Dr. Karan. A. K Moderator - Dr. Hemalatha .B.CDocument44 paginiAnti - VEGF Agents: Presenter - Dr. Karan. A. K Moderator - Dr. Hemalatha .B.CKaran Kumarswamy100% (1)
- Hutauruk CV 2019Document21 paginiHutauruk CV 2019HarisÎncă nu există evaluări
- Target IopDocument18 paginiTarget IopdrheriÎncă nu există evaluări
- M. Srinivasan - Keratitis-Intech (2012)Document70 paginiM. Srinivasan - Keratitis-Intech (2012)alex_andra_22Încă nu există evaluări
- Case Study GeriatricDocument4 paginiCase Study GeriatricJoshua HavanaÎncă nu există evaluări
- Management of Giant Retinal TearsDocument6 paginiManagement of Giant Retinal TearsAlejandro LondoñoÎncă nu există evaluări
- Normal Macular ThicknessDocument6 paginiNormal Macular ThicknessSara BkrÎncă nu există evaluări
- Shalakya Tantra SyllabusDocument65 paginiShalakya Tantra SyllabusIshwari GaikwadÎncă nu există evaluări
- Sense of VisionDocument34 paginiSense of VisionqqqqqÎncă nu există evaluări
- Retinopathy of PrematurityDocument30 paginiRetinopathy of Prematuritykenikirkucing2Încă nu există evaluări
- King Khaled Eye Specialist Hospital: Patient Referral FormDocument5 paginiKing Khaled Eye Specialist Hospital: Patient Referral Formفيصل الرباحÎncă nu există evaluări
- CXL Thin CorneaDocument10 paginiCXL Thin CorneaApps OmÎncă nu există evaluări
- Strabismus & Amblyopia: Dr. Boyke Sisprihattono, SPMDocument24 paginiStrabismus & Amblyopia: Dr. Boyke Sisprihattono, SPMPurnomo Ponco NugrohoÎncă nu există evaluări
- Geuder Annex II MDD CE 575415Document7 paginiGeuder Annex II MDD CE 575415sandesh.mhÎncă nu există evaluări
- MBBS PROF III PRE FINAL Catalogue Dec 2019 PDFDocument3 paginiMBBS PROF III PRE FINAL Catalogue Dec 2019 PDFAbeed PalÎncă nu există evaluări
- (OPHTHA) 7.1-Pediatric Ophthalmology-Strabismus and Amblyopia - Dr. AtienzaDocument14 pagini(OPHTHA) 7.1-Pediatric Ophthalmology-Strabismus and Amblyopia - Dr. AtienzaMaria Gracia YamsonÎncă nu există evaluări
- Essential Infantile Esotropia An Unusual Case ReportDocument3 paginiEssential Infantile Esotropia An Unusual Case ReportInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- Amblyopia: Glomarie Hope A. Paquera Danica Ilah M. SincoDocument39 paginiAmblyopia: Glomarie Hope A. Paquera Danica Ilah M. SincoJan IrishÎncă nu există evaluări
- 1 PBDocument4 pagini1 PBRian YupitaÎncă nu există evaluări
- 2006, Vol.19, Issues 4, Cataract Surgery in The New MillenniumDocument117 pagini2006, Vol.19, Issues 4, Cataract Surgery in The New MillenniumPatriciaChRistianiÎncă nu există evaluări
- Hong Kong Ophthalmological Symposium 2015 Abstract BookDocument44 paginiHong Kong Ophthalmological Symposium 2015 Abstract BookFaculty.Încă nu există evaluări
- TrachomaDocument17 paginiTrachomaArogya Raj De JosephÎncă nu există evaluări
- Ophthalmology 1.01 Introduction and History - Dr. Felarca and Dr. PimentelDocument3 paginiOphthalmology 1.01 Introduction and History - Dr. Felarca and Dr. PimentelMark AceÎncă nu există evaluări
- CHV Training - EYE BHojDocument129 paginiCHV Training - EYE BHojBhoja Raj GAUTAMÎncă nu există evaluări
- Hospital Email PhoneDocument2 paginiHospital Email PhoneNaveenJainÎncă nu există evaluări
- Basik Lasik - Tips On Lasik Eye SurgeryDocument4 paginiBasik Lasik - Tips On Lasik Eye Surgeryenglish-exactly100% (1)
- ARGOS® Swept Source OCT Biometer - P PUSC 0001Document24 paginiARGOS® Swept Source OCT Biometer - P PUSC 0001ANIEÎncă nu există evaluări
- List of Empanelled HCOs - Patna (Nov 2022)Document9 paginiList of Empanelled HCOs - Patna (Nov 2022)Shweta jainÎncă nu există evaluări
- Eyesight Without GlassesDocument8 paginiEyesight Without Glassesinfo-501699Încă nu există evaluări
- Laporan Kasus-Low Vision Dengan NystagmusDocument9 paginiLaporan Kasus-Low Vision Dengan NystagmusDony Dwi PutraÎncă nu există evaluări