S-ar putea să vă placă și
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- MRCS Essential ListDocument18 paginiMRCS Essential ListMahmoud Selim100% (1)
- Arterial Blood Gas AnalysisDocument20 paginiArterial Blood Gas AnalysisAdiantoÎncă nu există evaluări
- FDR - Vol 2 PDFDocument944 paginiFDR - Vol 2 PDFScott Hastings100% (2)
- Ketosis DMDocument33 paginiKetosis DMtiaÎncă nu există evaluări
- Renr Study GuideDocument57 paginiRenr Study GuideJerilee SoCute Watts92% (12)
- Management of Neonatal Hypothermia 3.0 PDFDocument14 paginiManagement of Neonatal Hypothermia 3.0 PDFNajwa binti MohdÎncă nu există evaluări
- BSC 2085 Anatomy and Physiology NCLEX Final Exam Predictor Study Guide (Verified and Correct Answers, 200 Questions Secure Highscore) Latest 2021Document131 paginiBSC 2085 Anatomy and Physiology NCLEX Final Exam Predictor Study Guide (Verified and Correct Answers, 200 Questions Secure Highscore) Latest 2021abbieÎncă nu există evaluări
- 10.6.09 Altman Lactic AcidosisDocument11 pagini10.6.09 Altman Lactic AcidosisCosmina Andreea TudoracheÎncă nu există evaluări
- Acid Blood Gas AnalysisDocument4 paginiAcid Blood Gas AnalysisG Aldanica Alburo MendozaÎncă nu există evaluări
- Annie - Acid Base BalanceDocument34 paginiAnnie - Acid Base BalanceAnnie GeorgeÎncă nu există evaluări
- No. 197b-Fetal Health SurveillanceDocument25 paginiNo. 197b-Fetal Health SurveillanceMaríaÎncă nu există evaluări
- Pre-Course MCQs - Mar 2008 - Corrected - PDFDocument8 paginiPre-Course MCQs - Mar 2008 - Corrected - PDFdeardiarymystery71% (17)
- Parenteral Nutrition CalculationsDocument62 paginiParenteral Nutrition CalculationsMohamad Samir100% (1)
- Emergency Medicine MnemonicsDocument18 paginiEmergency Medicine MnemonicsAnnapurna Dangeti100% (1)
- Major Intracellular and Extracellular IonsDocument20 paginiMajor Intracellular and Extracellular IonsTricia RestriveraÎncă nu există evaluări
- Infectious DiseaseDocument82 paginiInfectious DiseaseMedical videos67% (3)
- 2017 sepRECALLDocument58 pagini2017 sepRECALLkyahuaÎncă nu există evaluări
- Ug NotesDocument538 paginiUg NotesSteven IStudy SmithÎncă nu există evaluări
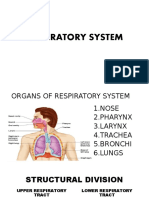
- Respiratory System LecDocument49 paginiRespiratory System LecStef FieÎncă nu există evaluări
- Blood Gas AnalysisDocument5 paginiBlood Gas AnalysisPathrecia Natalia SiagianÎncă nu există evaluări
- Types of CPRDocument12 paginiTypes of CPRSaid OmaryÎncă nu există evaluări
- Medical Surgical TransesDocument144 paginiMedical Surgical Transesmarlou agananÎncă nu există evaluări
- Daily Practice AnswersDocument37 paginiDaily Practice AnswersNazir AhmedÎncă nu există evaluări
- GeneralDocument31 paginiGeneralpikachu100% (1)
- L5 Buffer SolutionsDocument5 paginiL5 Buffer SolutionsanaÎncă nu există evaluări
- Basic Concepts of Fluid and Electrolyte TherapyDocument136 paginiBasic Concepts of Fluid and Electrolyte Therapymuhammad ajiÎncă nu există evaluări
- Metabolic Acidosis & AlkalosisDocument3 paginiMetabolic Acidosis & AlkalosisJared MabulayÎncă nu există evaluări
- Identifikasi Dini Pasien Kritis: Dr. Gatoet Soeseno, MARSDocument44 paginiIdentifikasi Dini Pasien Kritis: Dr. Gatoet Soeseno, MARSAviya EkutamiÎncă nu există evaluări
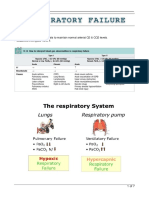
- Respiratory FailureDocument7 paginiRespiratory FailureLulu100% (1)
- Ruminal Acidosis.pdf - Google ДискDocument56 paginiRuminal Acidosis.pdf - Google ДискDVM 700Încă nu există evaluări