S-ar putea să vă placă și
- Seminar Topic: Biological Considerations in Maxillary ImpressionDocument17 paginiSeminar Topic: Biological Considerations in Maxillary ImpressionDrishti NagiÎncă nu există evaluări
- Posterior Palatal Seal: DR Muaiyed BuzayanDocument22 paginiPosterior Palatal Seal: DR Muaiyed BuzayanMuhammad Herry SeptianoorÎncă nu există evaluări
- Basic Principles in Impression Making M M DevanDocument6 paginiBasic Principles in Impression Making M M Devanmfaheemuddin85100% (1)
- Lingualized Occlusion ReviewDocument3 paginiLingualized Occlusion ReviewJessy ChenÎncă nu există evaluări
- Role of Tongue N Floor of Mouth in CD TRTDocument18 paginiRole of Tongue N Floor of Mouth in CD TRTashoorocksÎncă nu există evaluări
- 30-003. Devan, M.M. Basic Principles of Impression Making. J Prosthet Dent 2:26-35, 1952Document9 pagini30-003. Devan, M.M. Basic Principles of Impression Making. J Prosthet Dent 2:26-35, 1952Prashanth MarkaÎncă nu există evaluări
- Retention Support Stability CDDocument53 paginiRetention Support Stability CDAshraf GebreelÎncă nu există evaluări
- Finish LinesDocument17 paginiFinish LinesWaseem AhmedÎncă nu există evaluări
- Impression Techniques in RPDDocument82 paginiImpression Techniques in RPDpramodaniÎncă nu există evaluări
- Prostho IV Slide 3 Impression Making For Complete DenturesDocument82 paginiProstho IV Slide 3 Impression Making For Complete DenturesBoka BokaÎncă nu există evaluări
- Management of The Soft Palate Defect Steven Eckert PDFDocument15 paginiManagement of The Soft Palate Defect Steven Eckert PDFintanursamsiÎncă nu există evaluări
- Treatment of Grossly Resorbed Mandibular Ridge 1Document48 paginiTreatment of Grossly Resorbed Mandibular Ridge 1Faheemuddin Muhammad0% (1)
- Occlusion in Complete DentureDocument20 paginiOcclusion in Complete DentureBhushan ChavanÎncă nu există evaluări
- Aull. A Study of The Transverse Axis. (1963)Document11 paginiAull. A Study of The Transverse Axis. (1963)Jose Enrique AvilaÎncă nu există evaluări
- Occlusion in Complete DentureDocument43 paginiOcclusion in Complete DentureJaruwan Sae-IewÎncă nu există evaluări
- A Review On Posterior Palatal SealDocument6 paginiA Review On Posterior Palatal SealTanmay Srivastava100% (1)
- Posterior Palatal Seal ProsthoDocument64 paginiPosterior Palatal Seal ProsthoAmit BhargavÎncă nu există evaluări
- Lauritzen 1964Document10 paginiLauritzen 1964Priyanka GandhiÎncă nu există evaluări
- Neutral Zone Concept and TechniqueDocument6 paginiNeutral Zone Concept and TechniqueJasween KaurÎncă nu există evaluări
- Impression Procedures in CD - KIRTI SHARMADocument42 paginiImpression Procedures in CD - KIRTI SHARMAKirti SharmaÎncă nu există evaluări
- Orientation SonalDocument85 paginiOrientation Sonalsonalbatra100% (1)
- Maxillary ObturatorDocument79 paginiMaxillary ObturatorAmit KhattakÎncă nu există evaluări
- Cantor and Curtis ClassificationDocument4 paginiCantor and Curtis ClassificationMuhammad AwaisÎncă nu există evaluări
- Complete Denture Impression TechniquesDocument18 paginiComplete Denture Impression TechniquesYashpreetsingh BhatiaÎncă nu există evaluări
- Lingualised Occ RevisitedDocument5 paginiLingualised Occ RevisitedDrPrachi AgrawalÎncă nu există evaluări
- Implant Occlusion ppt4314Document43 paginiImplant Occlusion ppt4314Mostafa FayadÎncă nu există evaluări
- Eccentric RelationDocument10 paginiEccentric RelationKiana TediÎncă nu există evaluări
- Hobo Technique PDFDocument8 paginiHobo Technique PDFAmar BimavarapuÎncă nu există evaluări
- Complete Denture Impression TechniquesDocument14 paginiComplete Denture Impression TechniquesMahmoud BassiouniÎncă nu există evaluări
- Management of Compromised Residual Ridge PDFDocument73 paginiManagement of Compromised Residual Ridge PDFmarwa100% (1)
- Anatomical Landmarks and ImpressionDocument75 paginiAnatomical Landmarks and ImpressionSanjoy KarmakarÎncă nu există evaluări
- CLASSIC ARTICLE Clinical Measurement and EvaluationDocument5 paginiCLASSIC ARTICLE Clinical Measurement and EvaluationJesusCordoba100% (2)
- 04 - Interocclusal RecordsDocument15 pagini04 - Interocclusal RecordsCrina AmaliaÎncă nu există evaluări
- Horizontal Jaw RelationDocument101 paginiHorizontal Jaw Relationruchika0% (1)
- Intracoronal Restorations in FPDDocument60 paginiIntracoronal Restorations in FPDChandni SetiaÎncă nu există evaluări
- Complete dentures posterior palatal seal dimensions displacementDocument19 paginiComplete dentures posterior palatal seal dimensions displacementKrupali JainÎncă nu există evaluări
- Biological Considerations of Orientation, Vertical and Horizontal Jaw Relations in Complete Denture-First PartDocument43 paginiBiological Considerations of Orientation, Vertical and Horizontal Jaw Relations in Complete Denture-First PartArunÎncă nu există evaluări
- Complete Denture Construction Based On A Study Oflytle1959Document13 paginiComplete Denture Construction Based On A Study Oflytle1959Arun PrasadÎncă nu există evaluări
- Anatomy and Physiology in Relation To Complete Denture ConstructionDocument4 paginiAnatomy and Physiology in Relation To Complete Denture ConstructionCyril Almario CunananÎncă nu există evaluări
- Relining and Rebasing in Complete Dentures: Indian Dental AcademyDocument59 paginiRelining and Rebasing in Complete Dentures: Indian Dental AcademyNajeeb UllahÎncă nu există evaluări
- The Monoplane Occlusion For Complete Dentures: T H e SP Herical TheoryDocument7 paginiThe Monoplane Occlusion For Complete Dentures: T H e SP Herical TheorySahana RangarajanÎncă nu există evaluări
- Non-Rigid Connector Manages Pier AbutmentDocument3 paginiNon-Rigid Connector Manages Pier AbutmentIana RusuÎncă nu există evaluări
- The Use of Non Rigid Connectors in Fixed Partial Dentures With Pier Abutment: A Case ReportDocument4 paginiThe Use of Non Rigid Connectors in Fixed Partial Dentures With Pier Abutment: A Case ReportIOSRjournal100% (1)
- Connector Design PrinciplesDocument24 paginiConnector Design PrinciplesVikas Aggarwal100% (1)
- Occlusion in Complete Denture Part IIDocument48 paginiOcclusion in Complete Denture Part IIهجرسÎncă nu există evaluări
- Applied Anatomy Related To Complete Denture-Maxilla MandibleDocument57 paginiApplied Anatomy Related To Complete Denture-Maxilla MandibleRen Jye ChongÎncă nu există evaluări
- THE PROFILE PROSTHESIS: FIXED IMPLANT RESTORATIONDocument9 paginiTHE PROFILE PROSTHESIS: FIXED IMPLANT RESTORATIONSitiKhadijah100% (1)
- Principles of Tooth PreparationDocument3 paginiPrinciples of Tooth PreparationMarian TavassoliÎncă nu există evaluări
- Terminology of OcclusionDocument6 paginiTerminology of OcclusionShyam K MaharjanÎncă nu există evaluări
- RPD Impression TechniquesDocument34 paginiRPD Impression TechniquesKashish08100% (1)
- Occlusal Consideration For Mandibular Implant OverdenturesDocument12 paginiOcclusal Consideration For Mandibular Implant OverdenturesFrancisca Dinamarca Lama100% (1)
- Gothic Arch TracerDocument21 paginiGothic Arch TracerAnonymous ERJpRIr6WLÎncă nu există evaluări
- Restoration of THE Endodonticall Y Treated Tooth: Amith Babu Amrita Dora Ganesh O.R Praveen J Ourvind SinghDocument100 paginiRestoration of THE Endodonticall Y Treated Tooth: Amith Babu Amrita Dora Ganesh O.R Praveen J Ourvind SinghCahyani CahyaniÎncă nu există evaluări
- Horizontal Jaw Relation 1 1Document61 paginiHorizontal Jaw Relation 1 1Ankita SharmaÎncă nu există evaluări
- Fixed Orthodontic Appliances: A Practical GuideDe la EverandFixed Orthodontic Appliances: A Practical GuideEvaluare: 1 din 5 stele1/5 (1)
- Interpretation Basics of Cone Beam Computed TomographyDe la EverandInterpretation Basics of Cone Beam Computed TomographyEvaluare: 4 din 5 stele4/5 (1)
- Understanding Masticatory Function in Unilateral CrossbitesDe la EverandUnderstanding Masticatory Function in Unilateral CrossbitesÎncă nu există evaluări
- Dental Examination, Diagnosis and Treatment Planning GuideDocument28 paginiDental Examination, Diagnosis and Treatment Planning GuidefitsumÎncă nu există evaluări
- Essentials of ProsthodonticsDocument215 paginiEssentials of ProsthodonticsGenesis Centeno100% (5)
- Viva in Oral Surgery For Dental Students - Jaypee Brothers (2012) PDFDocument147 paginiViva in Oral Surgery For Dental Students - Jaypee Brothers (2012) PDFIsak Isak Isak0% (1)
- 174Document45 pagini174Steven RichardsÎncă nu există evaluări
- Complete Denture Cast Preparation GuideDocument18 paginiComplete Denture Cast Preparation Guidefitsum100% (1)
- Torrent Downloaded From Extratorrent - CCDocument1 paginăTorrent Downloaded From Extratorrent - CCcoolzatÎncă nu există evaluări
- Christian CredibilityDocument4 paginiChristian CredibilityfitsumÎncă nu există evaluări
- Articulators, Classification&AdjustmentDocument81 paginiArticulators, Classification&AdjustmentfitsumÎncă nu există evaluări
- Articulators, Classification&AdjustmentDocument81 paginiArticulators, Classification&AdjustmentfitsumÎncă nu există evaluări
- Face BowDocument81 paginiFace BowfitsumÎncă nu există evaluări
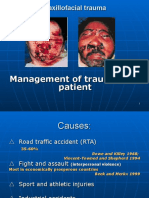
- Primary Management of Maxillofacial TraumaDocument34 paginiPrimary Management of Maxillofacial TraumafitsumÎncă nu există evaluări
- NAVLE Question of The DayDocument3 paginiNAVLE Question of The DayJuneyoung Lee100% (2)
- Principii Psiho OncologieDocument16 paginiPrincipii Psiho OncologieCristina Tulba100% (1)
- MPT Regulations and Syllabus for Tamil Nadu Medical UniversityDocument81 paginiMPT Regulations and Syllabus for Tamil Nadu Medical UniversitychandrusaiÎncă nu există evaluări
- Ot ProtocolDocument38 paginiOt ProtocolSelva KumarÎncă nu există evaluări
- Bped 100 Act 1Document2 paginiBped 100 Act 1DAVIE ELSISURAÎncă nu există evaluări
- Administration of Enema TechniquesDocument34 paginiAdministration of Enema TechniquesVishalni Menon Returnz100% (2)
- Water Soluble VitaminsDocument6 paginiWater Soluble VitaminsManjunatha HRÎncă nu există evaluări
- Key Statistics On Diabetes: Diabetes in The UK 2011/2012Document22 paginiKey Statistics On Diabetes: Diabetes in The UK 2011/2012Mark Anthony BetitoÎncă nu există evaluări
- Types: Guavas AreDocument12 paginiTypes: Guavas AreJesa Rose Tingson100% (1)
- FAST Protocol Provides Time-Sensitive Diagnosis in TraumaDocument103 paginiFAST Protocol Provides Time-Sensitive Diagnosis in TraumaSimina SerbanÎncă nu există evaluări
- DAFTAR ATC DDD ANTIBIOTIK WHO 2018 AbcDocument12 paginiDAFTAR ATC DDD ANTIBIOTIK WHO 2018 AbcMahezha DhewaÎncă nu există evaluări
- NH Medicaid Ambulance Medical NecessityDocument2 paginiNH Medicaid Ambulance Medical NecessityRolloTakesAWalkÎncă nu există evaluări
- Amway Platinums bulletin updates product pricingDocument4 paginiAmway Platinums bulletin updates product pricingSnehal Raut100% (1)
- Emailing 11. Dr. Manoj Gupta - Pelvic RT PlanningDocument69 paginiEmailing 11. Dr. Manoj Gupta - Pelvic RT PlanningafshanÎncă nu există evaluări
- Instructions For Use of Weight Watchers Body Fat Analysis Bathroom ScalesDocument2 paginiInstructions For Use of Weight Watchers Body Fat Analysis Bathroom Scalesjbloggs20070% (1)
- China GB4789.40 2010 Food Microbiological Examination Enterobacter Sakazakii PDFDocument13 paginiChina GB4789.40 2010 Food Microbiological Examination Enterobacter Sakazakii PDFmmoradi55Încă nu există evaluări
- Medical Tribune June 2012 PHDocument51 paginiMedical Tribune June 2012 PHAsmphLibrary OrtigasÎncă nu există evaluări
- Q A Random - 16Document8 paginiQ A Random - 16ja100% (1)
- Alsoufi 2018Document2 paginiAlsoufi 2018nidaakkusÎncă nu există evaluări
- Emilok 2011 MKT Plan TOTAL2Document19 paginiEmilok 2011 MKT Plan TOTAL2maawi2002yahoocomÎncă nu există evaluări
- Theories of LearningDocument112 paginiTheories of LearningPalak50% (2)
- Call The MidwifeDocument12 paginiCall The MidwifeCecilia DemergassoÎncă nu există evaluări
- Kawasaki Disease Definition and DiagnosisDocument3 paginiKawasaki Disease Definition and DiagnosisDavid ChengÎncă nu există evaluări
- Contoh Proposal Klinik Fisioterapi Di Puskesmas Jombatan JombangDocument4 paginiContoh Proposal Klinik Fisioterapi Di Puskesmas Jombatan JombangLuqmanul HakimÎncă nu există evaluări
- Tylenol and Thalidomide TragedyDocument29 paginiTylenol and Thalidomide TragedysiribandlaÎncă nu există evaluări
- Senthil Papers and BoardDocument4 paginiSenthil Papers and BoardRamakrishnan RajappanÎncă nu există evaluări
- H.4 Borderline PowerPoint Revised 2015Document31 paginiH.4 Borderline PowerPoint Revised 2015Ptrc Lbr LpÎncă nu există evaluări
- The Field of NROSDocument3 paginiThe Field of NROSXavier de lucaÎncă nu există evaluări
- Journal Pneumonia 1Document1 paginăJournal Pneumonia 1dwi-148502Încă nu există evaluări
- Oral Cavity Malignancy-SurgeryDocument62 paginiOral Cavity Malignancy-SurgeryAsif AbbasÎncă nu există evaluări