
S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- AnesthEssaysRes8168-2933181 004853 PDFDocument4 paginiAnesthEssaysRes8168-2933181 004853 PDFMerhan FoudaÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- CobasDocument145 paginiCobasAugia Nur IftihatunnisaÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- ALL Charity Clinical PDFDocument46 paginiALL Charity Clinical PDFMerhan FoudaÎncă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Operative Blood Transfusion Quality Improvement AuditDocument4 paginiOperative Blood Transfusion Quality Improvement AuditMerhan FoudaÎncă nu există evaluări
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Maintaining Constant Haemovigilance - Special Delivery Vol 66 Issue 2Document3 paginiMaintaining Constant Haemovigilance - Special Delivery Vol 66 Issue 2Merhan FoudaÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- WHO2013 BookDocument191 paginiWHO2013 BookMerhan FoudaÎncă nu există evaluări
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Planning and Designing A Hospital Transfusion Service - September 2016 - MedicalLab Management MagazineDocument5 paginiPlanning and Designing A Hospital Transfusion Service - September 2016 - MedicalLab Management MagazineMerhan FoudaÎncă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- 5th Handbook of Transfusion MedicineDocument186 pagini5th Handbook of Transfusion MedicineDokter Dhea Danni Agisty100% (1)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Contact: Risk Assessment &management, Contingency Planning, and Disaster/Crisis HandlingDocument1 paginăContact: Risk Assessment &management, Contingency Planning, and Disaster/Crisis HandlingMerhan FoudaÎncă nu există evaluări
- SAGM Blood For Neonatal Large Volume TransfusionDocument4 paginiSAGM Blood For Neonatal Large Volume TransfusionMerhan FoudaÎncă nu există evaluări
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Crossmatching, Types, Principle, Procedure and InterpretationDocument5 paginiCrossmatching, Types, Principle, Procedure and InterpretationMerhan FoudaÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Sree Chitra Tirunal Institute For Medical Science and TechnologyDocument103 paginiSree Chitra Tirunal Institute For Medical Science and TechnologyMerhan FoudaÎncă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- 2006 - ACUB HandbookDocument150 pagini2006 - ACUB HandbookMerhan FoudaÎncă nu există evaluări
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- 2006 - Egyptian National Blood Transfusion Transfusion StandardsDocument78 pagini2006 - Egyptian National Blood Transfusion Transfusion StandardsMerhan Fouda100% (1)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- 5th Handbook of Transfusion MedicineDocument186 pagini5th Handbook of Transfusion MedicineDokter Dhea Danni Agisty100% (1)
- Med Sun Appendix ADocument34 paginiMed Sun Appendix AMerhan FoudaÎncă nu există evaluări
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- A Guideline On Developing Effective Multiple Choice Questions and Construction of Single Best Answer FormatDocument8 paginiA Guideline On Developing Effective Multiple Choice Questions and Construction of Single Best Answer FormatMerhan FoudaÎncă nu există evaluări
- Hospital Feasibility Study PDFDocument115 paginiHospital Feasibility Study PDFMin Moe71% (7)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- 53 PDFDocument13 pagini53 PDFTemoteo L. Pupa III100% (1)
- Update and Utilization of Component Therapy in Blood TransfusionsDocument6 paginiUpdate and Utilization of Component Therapy in Blood TransfusionsMerhan FoudaÎncă nu există evaluări
- Directed DonationDocument3 paginiDirected DonationMerhan FoudaÎncă nu există evaluări
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Final Report enDocument395 paginiFinal Report enmejalliÎncă nu există evaluări
- Clonogenic Cell Survival AssayDocument9 paginiClonogenic Cell Survival AssayMerhan FoudaÎncă nu există evaluări
- Stability of NAT SamplesDocument8 paginiStability of NAT SamplesMerhan FoudaÎncă nu există evaluări
- Dipanjan Kumar Dey - Docx NewDocument6 paginiDipanjan Kumar Dey - Docx NewMerhan FoudaÎncă nu există evaluări
- Egypt National Blood Policy 2007Document44 paginiEgypt National Blood Policy 2007Merhan FoudaÎncă nu există evaluări
- Egypt National Blood Policy 2007Document44 paginiEgypt National Blood Policy 2007Merhan FoudaÎncă nu există evaluări
- National Standards 2007Document41 paginiNational Standards 2007Merhan FoudaÎncă nu există evaluări
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- 10 Chapter 3Document143 pagini10 Chapter 3Merhan FoudaÎncă nu există evaluări
- Targeted Immunization StrategiesDocument9 paginiTargeted Immunization StrategiesVernon MonteiroÎncă nu există evaluări
- Covid-19 Dashboard - Cases, Deaths and Vaccinations - New ScientistDocument5 paginiCovid-19 Dashboard - Cases, Deaths and Vaccinations - New Scientistchau chiÎncă nu există evaluări
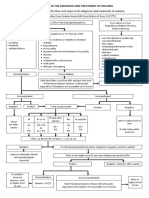
- Algorithm in The Diagnosis and Treatment of MalariaDocument1 paginăAlgorithm in The Diagnosis and Treatment of MalariaPearl Monette Cedeño AngÎncă nu există evaluări
- Erythromycin & Pneumococcal VaccineDocument6 paginiErythromycin & Pneumococcal VaccineNikki Joy NavarroÎncă nu există evaluări
- Cefuroxime (Drug Study)Document2 paginiCefuroxime (Drug Study)Franz.thenurse6888100% (13)
- Guide To Biologic Therapy 1Document24 paginiGuide To Biologic Therapy 1Andra GarbeaÎncă nu există evaluări
- Autoimmune Hemolytic Anemia in Adults 2019 PDFDocument22 paginiAutoimmune Hemolytic Anemia in Adults 2019 PDFKevin Mora BañosÎncă nu există evaluări
- Elsevier's Integrated Pathology Volume 1 issue 1 2006 [doi 10.1016_B978-0-323-04328-1.50008-5] King, Thomas C. -- Elsevier's Integrated Pathology __ Inflammation, Inflammatory Mediators, and Immune-.pdfDocument37 paginiElsevier's Integrated Pathology Volume 1 issue 1 2006 [doi 10.1016_B978-0-323-04328-1.50008-5] King, Thomas C. -- Elsevier's Integrated Pathology __ Inflammation, Inflammatory Mediators, and Immune-.pdfdaniel satyoÎncă nu există evaluări
- Immunology Janis Kuby .Page001Document1 paginăImmunology Janis Kuby .Page001microkannanÎncă nu există evaluări
- Diseases Affecting Pregnancy: (Tuberculosis & STD)Document64 paginiDiseases Affecting Pregnancy: (Tuberculosis & STD)Cyrelle Jen TorresÎncă nu există evaluări
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Communicable Diseases: HIV PositiveDocument20 paginiCommunicable Diseases: HIV Positivepinoy_nurse100% (1)
- Hla Typing and Cross Match: Shashi AnandDocument26 paginiHla Typing and Cross Match: Shashi AnandDil NavabÎncă nu există evaluări
- Biology Ebola Virus Project ReportDocument19 paginiBiology Ebola Virus Project ReportChaitaneyMorÎncă nu există evaluări
- Clinical Bacteriology by DR Agwu EzeraDocument116 paginiClinical Bacteriology by DR Agwu EzeraRodgers Bazigu100% (1)
- Pign Vs Irgn: by DR Monika Resident Nephrology, Saveetha CollegeDocument50 paginiPign Vs Irgn: by DR Monika Resident Nephrology, Saveetha CollegeDr MonikaÎncă nu există evaluări
- Wanger A, Chavez V, Huang R, Wahed A, Dasgupta A, Actor J. 2017. Microbiology and Molecular Diagnosis in Pathology. Camridge (US) Academic Press.Document12 paginiWanger A, Chavez V, Huang R, Wahed A, Dasgupta A, Actor J. 2017. Microbiology and Molecular Diagnosis in Pathology. Camridge (US) Academic Press.Annisa YohanesÎncă nu există evaluări
- Iga Nephropathy and Vasculitis: Dr. Rida Malik Nephrology ResidentDocument52 paginiIga Nephropathy and Vasculitis: Dr. Rida Malik Nephrology ResidentDr Rida And Shoaib VideosÎncă nu există evaluări
- Epstein-Barr Virus Infections in PatientsDocument3 paginiEpstein-Barr Virus Infections in PatientsFilipos ConstantinÎncă nu există evaluări
- Lecture 13 Tumor ImmunologyDocument99 paginiLecture 13 Tumor Immunologyمحمود محمد100% (1)
- Clinical Manifestation:: Medical ManagementDocument5 paginiClinical Manifestation:: Medical ManagementChristina BarrogaÎncă nu există evaluări
- 4life Transfer Factor: Which Product Is Right For Me?Document1 pagină4life Transfer Factor: Which Product Is Right For Me?jhimsyÎncă nu există evaluări
- Literasi Bahasa Inggris - 260124Document2 paginiLiterasi Bahasa Inggris - 260124abcdefvinsÎncă nu există evaluări
- Micro 5Document51 paginiMicro 5NeviÎncă nu există evaluări
- Infectious DiseaseDocument81 paginiInfectious DiseaseAmit Gandhi67% (3)
- Systemic Lupus ErythematosusDocument64 paginiSystemic Lupus Erythematosusganga2424100% (1)
- Allergic Rhinitis Brochure ContentDocument2 paginiAllergic Rhinitis Brochure ContentWenalyn Grace Abella LlavanÎncă nu există evaluări
- Ch2 InflamDocument49 paginiCh2 InflamleartaÎncă nu există evaluări
- Hawassa University Department of Biotechnology: We Strive For Wisdom Chapter-3Document26 paginiHawassa University Department of Biotechnology: We Strive For Wisdom Chapter-3AZ Amanii BossÎncă nu există evaluări
- Case Report Generalized Dermatophytosis in Six Yorkshire Terrier DogsDocument7 paginiCase Report Generalized Dermatophytosis in Six Yorkshire Terrier DogsjenÎncă nu există evaluări
- 4-Overview of HIV AIDS - LAC - Dr. Ethyl DanoDocument29 pagini4-Overview of HIV AIDS - LAC - Dr. Ethyl DanoNiccolo G. ChiongbianÎncă nu există evaluări
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDe la EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDEvaluare: 5 din 5 stele5/5 (2)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDe la EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityEvaluare: 4 din 5 stele4/5 (28)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDe la EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionEvaluare: 4 din 5 stele4/5 (404)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDe la EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeEvaluare: 2 din 5 stele2/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDe la EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedEvaluare: 5 din 5 stele5/5 (81)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDe la EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Gut: the new and revised Sunday Times bestsellerDe la EverandGut: the new and revised Sunday Times bestsellerEvaluare: 4 din 5 stele4/5 (393)





































































![Elsevier's Integrated Pathology Volume 1 issue 1 2006 [doi 10.1016_B978-0-323-04328-1.50008-5] King, Thomas C. -- Elsevier's Integrated Pathology __ Inflammation, Inflammatory Mediators, and Immune-.pdf](https://imgv2-2-f.scribdassets.com/img/document/452619367/149x198/44e4142005/1584787257?v=1)


























