S-ar putea să vă placă și
- HSE Statistics PDFDocument5 paginiHSE Statistics PDFRashid100% (1)
- SASO Standards ListDocument5 paginiSASO Standards ListRashidÎncă nu există evaluări
- SASO StandardsDocument73 paginiSASO StandardsLloyd R. Ponce50% (4)
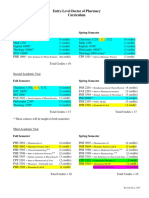
- Pharmd CurriculumDocument18 paginiPharmd Curriculum5377773Încă nu există evaluări
- Process Flow Diagram: Avon Tubetech Pvt. Limited, FaridabadDocument4 paginiProcess Flow Diagram: Avon Tubetech Pvt. Limited, FaridabadHimanshu GaurÎncă nu există evaluări
- QSP-01 Control of Docs Internal OriginDocument3 paginiQSP-01 Control of Docs Internal OriginDhinakaranÎncă nu există evaluări
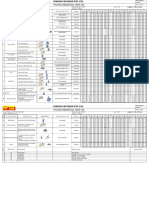
- Competency MappingDocument38 paginiCompetency MappingprashanthÎncă nu există evaluări
- Die Inward Inspection ReportDocument2 paginiDie Inward Inspection ReportRahul DevkateÎncă nu există evaluări
- OPL Bolt TighteningDocument2 paginiOPL Bolt TighteningmmkattaÎncă nu există evaluări
- Rimal Global Technical Services LLC.: HSE Management System ProcedureDocument1 paginăRimal Global Technical Services LLC.: HSE Management System ProcedureSreekumarÎncă nu există evaluări
- Butterworth Feedmill SDN BHD: Toolbox Meeting RecordsDocument1 paginăButterworth Feedmill SDN BHD: Toolbox Meeting RecordsNurul NatashaÎncă nu există evaluări
- OeeDocument16 paginiOeeRohtash fastnerÎncă nu există evaluări
- FIR-garments PDFDocument4 paginiFIR-garments PDFTarun PariharÎncă nu există evaluări
- ICAS Initial-Capacity-Assessment-Sheet 2010-12-09Document15 paginiICAS Initial-Capacity-Assessment-Sheet 2010-12-09Fitzi ShadyÎncă nu există evaluări
- Internal Rejection LevelDocument1 paginăInternal Rejection LevelISO CERTIFICATION-ROHSÎncă nu există evaluări
- Control Plan: Pre-Launch Production PrototypeDocument1 paginăControl Plan: Pre-Launch Production PrototypeAnkur DhirÎncă nu există evaluări
- IFI Safety Statement August 2017Document527 paginiIFI Safety Statement August 2017BryanÎncă nu există evaluări
- Management Programme (Hsmp/emp)Document1 paginăManagement Programme (Hsmp/emp)midozotyÎncă nu există evaluări
- Legal Register 01Document7 paginiLegal Register 01jithin shankarÎncă nu există evaluări
- Fire Risk Assessment - JRG Automotive Industries India Pvt. Ltd. (J253)Document8 paginiFire Risk Assessment - JRG Automotive Industries India Pvt. Ltd. (J253)neerajrdxÎncă nu există evaluări
- OCP - 15 - GrindingDocument2 paginiOCP - 15 - GrindingNagendra Kumar SinghÎncă nu există evaluări
- Iso 1083 2018Document13 paginiIso 1083 2018Kerem ErtemÎncă nu există evaluări
- RoHS BrasileiraDocument39 paginiRoHS BrasileiraLuis ReisÎncă nu există evaluări
- P O S T (Post) : Ositive Perational Afety Arget Score CardDocument2 paginiP O S T (Post) : Ositive Perational Afety Arget Score CardekoimampÎncă nu există evaluări
- Sub Vendor Audit Checklist-PersonnelDocument5 paginiSub Vendor Audit Checklist-PersonnelaszlizaÎncă nu există evaluări
- Shopfloor Monitoring ChecklistDocument1 paginăShopfloor Monitoring ChecklistSafety DeptÎncă nu există evaluări
- Setco Automotive LTD.: Weekly Production PlanningDocument2 paginiSetco Automotive LTD.: Weekly Production PlanningDisha ShahÎncă nu există evaluări
- MSA FormatDocument4 paginiMSA FormatSaurabh PhandÎncă nu există evaluări
- Sundram Fasteners LTD, Autolec Division. Apqp Timing Plan - XXXXXXXXXXX (1111111) Date: XX - XX.XXXXDocument2 paginiSundram Fasteners LTD, Autolec Division. Apqp Timing Plan - XXXXXXXXXXX (1111111) Date: XX - XX.XXXXUdhayakumarÎncă nu există evaluări
- 3 3bb0aDocument7 pagini3 3bb0aEleandro JoaquimÎncă nu există evaluări
- NSA Audit ReportDocument6 paginiNSA Audit ReportNaveen GuptaÎncă nu există evaluări
- Hi-Tech Engineers: Daily Safety CrossDocument12 paginiHi-Tech Engineers: Daily Safety CrossMohit SinghÎncă nu există evaluări
- Performance Management System Ip PDFDocument11 paginiPerformance Management System Ip PDFsahib singhÎncă nu există evaluări
- Facility Health, Safety and Environmental Management (Hse)Document2 paginiFacility Health, Safety and Environmental Management (Hse)Syahirah NazriÎncă nu există evaluări
- Quality Plan (Incoming) : Assy / Sub-Assy Name: Format No: Assy / Sub-Assy No: Latest Drawing Reference DetailsDocument5 paginiQuality Plan (Incoming) : Assy / Sub-Assy Name: Format No: Assy / Sub-Assy No: Latest Drawing Reference DetailsScientific KingÎncă nu există evaluări
- Management Review Programme (Insert Year) : ISO 9001:2015 QMSDocument2 paginiManagement Review Programme (Insert Year) : ISO 9001:2015 QMSFrench Sarah NeraÎncă nu există evaluări
- Work Instructions Work Instructions: Display Standard-Assembly & FirewallDocument7 paginiWork Instructions Work Instructions: Display Standard-Assembly & Firewallshobha shelarÎncă nu există evaluări
- Enquiry Review Check ListDocument1 paginăEnquiry Review Check ListMuthuÎncă nu există evaluări
- 1.1 SMP For Mechanical Maintance of AirtubeDocument2 pagini1.1 SMP For Mechanical Maintance of AirtubePRANAV KUMAR GAUTAMÎncă nu există evaluări
- PFD - Example..Document4 paginiPFD - Example..lalit GuptaÎncă nu există evaluări
- Kansal Industries - Tool Development Plan Model 'N': Assy T0 SampleDocument2 paginiKansal Industries - Tool Development Plan Model 'N': Assy T0 SampleajayÎncă nu există evaluări
- Fire Extinguisher Check SheetDocument5 paginiFire Extinguisher Check SheetSafety DeptÎncă nu există evaluări
- Nabtesco - Annual Appraisal Sheet (For Manager & Above) 2021Document10 paginiNabtesco - Annual Appraisal Sheet (For Manager & Above) 2021Kiran AmboreÎncă nu există evaluări
- D7029 - Supplier Inspection Report FormatDocument4 paginiD7029 - Supplier Inspection Report Formatnisha_khanÎncă nu există evaluări
- Central EHS TemplateDocument4 paginiCentral EHS Templateakshay aryaÎncă nu există evaluări
- FT 35 DC D10447340A Process SheetDocument7 paginiFT 35 DC D10447340A Process SheetSuraj RawatÎncă nu există evaluări
- F HR 20 Skill Approved ListDocument6 paginiF HR 20 Skill Approved ListRohtash fastnerÎncă nu există evaluări
- Work Permit ProcedureDocument2 paginiWork Permit Procedureवात्सल्य कृतार्थÎncă nu există evaluări
- 02 AS-F-HSE 002B - HSE InductionTraining.Document1 pagină02 AS-F-HSE 002B - HSE InductionTraining.JHUPEL ABARIALÎncă nu există evaluări
- Appendix - 9 - APQP - Timing - PlanDocument1 paginăAppendix - 9 - APQP - Timing - PlanChandru JattiÎncă nu există evaluări
- Chennai Radha Engineering Works (P) LTD.: Near Miss / Incident Report & Investigation FormDocument2 paginiChennai Radha Engineering Works (P) LTD.: Near Miss / Incident Report & Investigation FormsamÎncă nu există evaluări
- Actual Sampling PlanDocument2 paginiActual Sampling PlanAtlasLiu100% (1)
- 8 D For ShrinkageDocument6 pagini8 D For ShrinkageSachin KumbharÎncă nu există evaluări
- WI-R&D-33 - Field Validation of ClutchDocument3 paginiWI-R&D-33 - Field Validation of ClutchDisha ShahÎncă nu există evaluări
- Revision StatusDocument1 paginăRevision Statussasi10000Încă nu există evaluări
- Preventive Maintenance Check List: (Legend: / Due, X Done)Document2 paginiPreventive Maintenance Check List: (Legend: / Due, X Done)Rohtash fastnerÎncă nu există evaluări
- SACL Supplier Facility Audit (Summary) : Not ApprovedDocument13 paginiSACL Supplier Facility Audit (Summary) : Not ApprovedShankar ChowdhuryÎncă nu există evaluări
- IM 12 EHS Risk Management ProcedureDocument166 paginiIM 12 EHS Risk Management Procedureharish14586100% (1)
- Format No - Qf-As-02 - Daily Production Log BookDocument2 paginiFormat No - Qf-As-02 - Daily Production Log BookDisha ShahÎncă nu există evaluări
- 66 FM-TRD-05 Tool History CardDocument2 pagini66 FM-TRD-05 Tool History CardUttrakhand Vibes- OriginalÎncă nu există evaluări
- 5S Checklist & Rota New 08Document1 pagină5S Checklist & Rota New 08akbars.thasimaÎncă nu există evaluări
- Haccp Documents 1Document26 paginiHaccp Documents 1olivia domingoÎncă nu există evaluări
- Form E2 - Government Entity Quarterly Performance Report-V3.0 EnglishDocument3 paginiForm E2 - Government Entity Quarterly Performance Report-V3.0 EnglishsamuelÎncă nu există evaluări
- Form E - Entity Quarterly Performance Report - V3.0 EnglishDocument3 paginiForm E - Entity Quarterly Performance Report - V3.0 Englishsamuel100% (2)
- The Health and Safety (Display Screen Equipment) Regulations 1992Document9 paginiThe Health and Safety (Display Screen Equipment) Regulations 1992RashidÎncă nu există evaluări
- Cleaning Master ScheduleDocument1 paginăCleaning Master ScheduleRashidÎncă nu există evaluări
- Sample: Hearing Loss Prevention ProgramDocument8 paginiSample: Hearing Loss Prevention ProgramRashidÎncă nu există evaluări
- ISO 18001 ChecklistDocument6 paginiISO 18001 ChecklistRashid100% (1)
- Part1 5Document4 paginiPart1 5RashidÎncă nu există evaluări
- Accident-Incident Report FormDocument1 paginăAccident-Incident Report FormKrishna SrikanthÎncă nu există evaluări
- Accident-Incident Report FormDocument1 paginăAccident-Incident Report FormKrishna SrikanthÎncă nu există evaluări
- 3S HSE MS Docs ContentDocument85 pagini3S HSE MS Docs Contentrashid zamanÎncă nu există evaluări
- Consequences 0 A B C: Low Risk Medium Risk High RiskDocument3 paginiConsequences 0 A B C: Low Risk Medium Risk High Riskrashid zamanÎncă nu există evaluări
- Iso 9001-2008Document40 paginiIso 9001-2008rashid zamanÎncă nu există evaluări
- ISO 18001 ChecklistDocument6 paginiISO 18001 ChecklistRashid100% (1)
- Industrial Internet of Things: Presented To-Presented byDocument18 paginiIndustrial Internet of Things: Presented To-Presented byGaurav RaturiÎncă nu există evaluări
- Dizziness - Vertigo and HomoeopathyDocument38 paginiDizziness - Vertigo and HomoeopathyDr. Rajneesh Kumar Sharma MD HomÎncă nu există evaluări
- Eating With Chloe Lets EatDocument150 paginiEating With Chloe Lets Eatemily.jarrodÎncă nu există evaluări
- Trends in FoodDocument3 paginiTrends in FoodAliÎncă nu există evaluări
- Sample Dilapidation ReportDocument8 paginiSample Dilapidation ReportczarusÎncă nu există evaluări
- Ventricular Septal DefectDocument9 paginiVentricular Septal DefectpepotchÎncă nu există evaluări
- AD1 Elements of Architectural Composition For Placemaking PDFDocument4 paginiAD1 Elements of Architectural Composition For Placemaking PDFAndre Yap100% (1)
- Rac Question PaperDocument84 paginiRac Question PaperibrahimÎncă nu există evaluări
- BTK Implant Guide SurgeryDocument48 paginiBTK Implant Guide SurgeryMaria VolvinaÎncă nu există evaluări
- Uji Efektivitas Mikroba Rumpun BambuDocument7 paginiUji Efektivitas Mikroba Rumpun BambuUse Real ProjectÎncă nu există evaluări
- DEEP ECOLOGY - An Intro - McLaughlinDocument5 paginiDEEP ECOLOGY - An Intro - McLaughlinCarlo MagcamitÎncă nu există evaluări
- BECO UACE Chem2Document6 paginiBECO UACE Chem2EMMANUEL BIRUNGIÎncă nu există evaluări
- The Unofficial Aterlife GuideDocument33 paginiThe Unofficial Aterlife GuideIsrael Teixeira de AndradeÎncă nu există evaluări
- Angewandte: ChemieDocument13 paginiAngewandte: ChemiemilicaÎncă nu există evaluări
- St. John's Wort: Clinical OverviewDocument14 paginiSt. John's Wort: Clinical OverviewTrismegisteÎncă nu există evaluări
- All Pop SongsDocument53 paginiAll Pop SongsMadeleneQuiogueÎncă nu există evaluări
- The Wilson Quarterly: The World's New Numbers by Martin WalkerDocument13 paginiThe Wilson Quarterly: The World's New Numbers by Martin WalkerDavid WeekÎncă nu există evaluări
- Pref - 2 - Grammar 1.2 - Revisión Del IntentoDocument2 paginiPref - 2 - Grammar 1.2 - Revisión Del IntentoJuan M. Suarez ArevaloÎncă nu există evaluări
- Contact Inform 2002 PDFDocument24 paginiContact Inform 2002 PDFFrank AlmeidaÎncă nu există evaluări
- Cell Wall Synthesis InhibitorsDocument6 paginiCell Wall Synthesis InhibitorsRPh Krishna Chandra JagritÎncă nu există evaluări
- UC Lennox Serie 13 Acx Merit R-410aDocument52 paginiUC Lennox Serie 13 Acx Merit R-410ajmurcia80Încă nu există evaluări
- Class 12 - Maths - MatricesDocument87 paginiClass 12 - Maths - MatricesAishwarya MishraÎncă nu există evaluări
- VTA28-G5: Fuel OptimizedDocument3 paginiVTA28-G5: Fuel OptimizedIslam HemdanÎncă nu există evaluări
- Sci NB Mod 2 LSN 3Document4 paginiSci NB Mod 2 LSN 3Ramses octavio Rodriguez ocanasÎncă nu există evaluări
- 412 X 7 Va CJ CSDocument1 pagină412 X 7 Va CJ CSRajesh KumarÎncă nu există evaluări
- Germania Agenturinfo enDocument4 paginiGermania Agenturinfo enДушан СтепановићÎncă nu există evaluări
- Future AncestorsDocument44 paginiFuture AncestorsAlex100% (1)
- Yadea User Manual For e Scooter 1546004910Document44 paginiYadea User Manual For e Scooter 1546004910Danthe ThenadÎncă nu există evaluări
- TranscriptDocument1 paginăTranscriptapi-310448954Încă nu există evaluări