S-ar putea să vă placă și
- Math Practice Problems Group 3Document2 paginiMath Practice Problems Group 3Lukman Nal 26Încă nu există evaluări
- BMC Transitions of CareDocument2 paginiBMC Transitions of Carebalab2311Încă nu există evaluări
- MACHNISM OF NURSING DRUG NAME INDICATIOONDocument2 paginiMACHNISM OF NURSING DRUG NAME INDICATIOONsalwaÎncă nu există evaluări
- AcetaminophenDocument2 paginiAcetaminophendrugcardref100% (1)
- MucosolvanDocument2 paginiMucosolvanAyah Paasa100% (1)
- Types of Insulin According to Mode of ActionDocument1 paginăTypes of Insulin According to Mode of ActionAssem Ashraf Khidhr100% (1)
- Drug StudyDocument16 paginiDrug StudyMonica Luz FajardoÎncă nu există evaluări
- Drug Study: Far Eastern UniversityDocument3 paginiDrug Study: Far Eastern UniversityChoy DacanayÎncă nu există evaluări
- Salbuterol Generic NameDocument4 paginiSalbuterol Generic NamejunieÎncă nu există evaluări
- Medication DilutionDocument22 paginiMedication DilutionYaser Salman100% (1)
- CVD HypertensionDocument15 paginiCVD HypertensionAbigail BascoÎncă nu există evaluări
- Bariatric Surgery Nutrition GuideDocument35 paginiBariatric Surgery Nutrition GuideMoitri ChatterjeeÎncă nu există evaluări
- First Aide 2023Document97 paginiFirst Aide 2023jrfdcafprescomÎncă nu există evaluări
- Module 3 Activity 2 Drug Study Ciprofloxacin PaxilDocument6 paginiModule 3 Activity 2 Drug Study Ciprofloxacin PaxilEugene MananganÎncă nu există evaluări
- Acute Poisoning of Therapeutic Agents: by Alemayehu TomaDocument42 paginiAcute Poisoning of Therapeutic Agents: by Alemayehu TomaYohannis AsefaÎncă nu există evaluări
- Metoprolol Teaching PlanDocument18 paginiMetoprolol Teaching Planapi-419091662Încă nu există evaluări
- Formulas and DripsDocument6 paginiFormulas and DripsJsohna BelinaÎncă nu există evaluări
- Classification of Burns Based On Depth CharacteristicsDocument2 paginiClassification of Burns Based On Depth CharacteristicsmexelleÎncă nu există evaluări
- Critical Care of Hyperglycemic Hyperosmolar Syndrome (HHNSDocument4 paginiCritical Care of Hyperglycemic Hyperosmolar Syndrome (HHNSJan Crizza Dale R. FrancoÎncă nu există evaluări
- San Beda College College of Nursing drug study guideDocument3 paginiSan Beda College College of Nursing drug study guideaycee0316Încă nu există evaluări
- Endocrine System: (General Key Points)Document32 paginiEndocrine System: (General Key Points)susan2johnson-501300Încă nu există evaluări
- The Musculoskeletal HandoutsDocument3 paginiThe Musculoskeletal Handouts_Advernice_Încă nu există evaluări
- NCM 118a Lec 9 Liver FailureDocument9 paginiNCM 118a Lec 9 Liver FailureJan Crizza Dale R. FrancoÎncă nu există evaluări
- RHEUMATOID ARTHYRITIS CASEDocument32 paginiRHEUMATOID ARTHYRITIS CASEJune Faith HacheroÎncă nu există evaluări
- GIT Individual Case StudyDocument13 paginiGIT Individual Case StudyKirito Dokkie100% (1)
- Assessment by Body SystemsDocument2 paginiAssessment by Body SystemsPat McGarryÎncă nu există evaluări
- Asthma and PneumoniaDocument121 paginiAsthma and PneumoniaPaula AbilÎncă nu există evaluări
- J.S Case Study 1 PDFDocument2 paginiJ.S Case Study 1 PDFania ojedaÎncă nu există evaluări
- Carbetocin For The Prevention of Postpartum Hemorrhage A Systematic ReviewDocument7 paginiCarbetocin For The Prevention of Postpartum Hemorrhage A Systematic ReviewOscar Gregorio Coronado MacdanielÎncă nu există evaluări
- Drug Name Mechanism of Action Dosage Indication Contraindication Side Effects/ Adverse Effects Nursing ResponsibilitiesDocument4 paginiDrug Name Mechanism of Action Dosage Indication Contraindication Side Effects/ Adverse Effects Nursing ResponsibilitiesKat BausaÎncă nu există evaluări
- Intake & Output Monitoring Sheet: 11 PM 11-7 1000 ML 0 550 ML 0 0Document2 paginiIntake & Output Monitoring Sheet: 11 PM 11-7 1000 ML 0 550 ML 0 0Renea Joy ArruejoÎncă nu există evaluări
- Drug StudyDocument8 paginiDrug StudyJay-ar Batara SorianoÎncă nu există evaluări
- Taking Blood Pressure ManuallyDocument2 paginiTaking Blood Pressure ManuallyManoj Kumar GÎncă nu există evaluări
- SH CP 17 Zuclopenthixol Acetate GuidelinesxDocument8 paginiSH CP 17 Zuclopenthixol Acetate Guidelinesxlight002Încă nu există evaluări
- Hips Back Ankles Buttocks HeelsDocument13 paginiHips Back Ankles Buttocks Heelsفرزدق الحسيناويÎncă nu există evaluări
- Narrative PathophysiologyDocument5 paginiNarrative Pathophysiologymyer pasandalanÎncă nu există evaluări
- Final NCPDocument5 paginiFinal NCPAce VirtusioÎncă nu există evaluări
- Pathophysiology - Tia VS CvaDocument6 paginiPathophysiology - Tia VS CvaZeo Zafaralla100% (1)
- Atenolol TenorminDocument3 paginiAtenolol TenorminLIEZEL GRACE VELAYOÎncă nu există evaluări
- Haloperidol PDFDocument1 paginăHaloperidol PDFAda AlvarezÎncă nu există evaluări
- Drug StudyDocument2 paginiDrug Studyunkown userÎncă nu există evaluări
- Palliative Care Case Study: Qamar Abbas Deputy Medical Director ST Clare HospiceDocument12 paginiPalliative Care Case Study: Qamar Abbas Deputy Medical Director ST Clare HospicePraba KaranÎncă nu există evaluări
- Drug Used in VomitingDocument1 paginăDrug Used in VomitingSyamil AizatÎncă nu există evaluări
- What Is Radioactive PollutionDocument4 paginiWhat Is Radioactive PollutionJoy MitraÎncă nu există evaluări
- Nursing Assessment IIDocument5 paginiNursing Assessment IImyer pasandalanÎncă nu există evaluări
- Intr Oduction: Classification of PainDocument4 paginiIntr Oduction: Classification of Painanimesh panda100% (1)
- ACLS Simplify AlgorithmDocument6 paginiACLS Simplify AlgorithmKristine Monforte Coma UritaÎncă nu există evaluări
- Drug StudyDocument7 paginiDrug Studyanne009Încă nu există evaluări
- Amlodipine Captopril MetronidazoleDocument5 paginiAmlodipine Captopril Metronidazolekhrysty1506Încă nu există evaluări
- ACLS AgorithmDocument55 paginiACLS AgorithmkpsuanÎncă nu există evaluări
- Appendix A: Sample Patient Profiles and Prescriptions: (For Pharmacist Use)Document6 paginiAppendix A: Sample Patient Profiles and Prescriptions: (For Pharmacist Use)Cesly Jewel Acosta AvilesÎncă nu există evaluări
- Duloxetine PDFDocument4 paginiDuloxetine PDFscribdseewalÎncă nu există evaluări
- Autonomic HyperreflexiaDocument3 paginiAutonomic HyperreflexiaGibe BebitaÎncă nu există evaluări
- 8 Pulseless Arrest OkDocument33 pagini8 Pulseless Arrest OkJulienne CaoileÎncă nu există evaluări
- Multiple Sclerosis PDFDocument1 paginăMultiple Sclerosis PDFAcey TfÎncă nu există evaluări
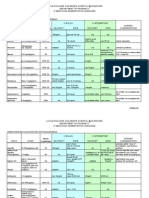
- Flores Mary Jane Generic Drug ChartDocument23 paginiFlores Mary Jane Generic Drug ChartKristine Dela CruzÎncă nu există evaluări
- Spinal Vs Neuro ShockDocument1 paginăSpinal Vs Neuro ShockLiza Kamelia100% (2)
- Drug Therapy of DM - Oral Antidiabetic DrugsDocument3 paginiDrug Therapy of DM - Oral Antidiabetic DrugsSurria Suguna15Încă nu există evaluări
- Anti Diabetik Oral Dan InsulinDocument97 paginiAnti Diabetik Oral Dan InsulinSuci AlimaÎncă nu există evaluări
- Diabetes MellitusDocument6 paginiDiabetes Mellitusmaham jahangirÎncă nu există evaluări
- Urinary Concentration and DilutionDocument10 paginiUrinary Concentration and DilutionAbhineeth BhatÎncă nu există evaluări
- Unit 2 Histo Study GuideDocument2 paginiUnit 2 Histo Study GuideAbhineeth BhatÎncă nu există evaluări
- VocabDocument4 paginiVocabAbhineeth BhatÎncă nu există evaluări
- Gi HyDocument2 paginiGi HyAbhineeth BhatÎncă nu există evaluări
- Step 1 PlanDocument6 paginiStep 1 PlanUma MounaÎncă nu există evaluări
- 2017 Fas1 Errata MarchDocument4 pagini2017 Fas1 Errata MarchФеденко ЭдуардÎncă nu există evaluări
- Usmle Hy Step1Document20 paginiUsmle Hy Step1Sindu SaiÎncă nu există evaluări
- STEP1 ResourcesDocument2 paginiSTEP1 ResourcesAbhineeth BhatÎncă nu există evaluări
- Guide To BoardsDocument3 paginiGuide To BoardsAbhineeth BhatÎncă nu există evaluări
- PathologyDocument54 paginiPathologyAli Abbas100% (8)
- GuideDocument16 paginiGuideAbhineeth BhatÎncă nu există evaluări
- DM2Document12 paginiDM2Abhineeth BhatÎncă nu există evaluări
- Approved: HFHS Nov-June Only HFH Has No PrerequisitesDocument1 paginăApproved: HFHS Nov-June Only HFH Has No PrerequisitesAbhineeth BhatÎncă nu există evaluări
- Guide PDDocument2 paginiGuide PDAbhineeth BhatÎncă nu există evaluări
- First SpeakerDocument2 paginiFirst SpeakerAbhineeth BhatÎncă nu există evaluări
- Notion of Narrative Based On Whats Dominant in End of Life StoriesDocument1 paginăNotion of Narrative Based On Whats Dominant in End of Life StoriesAbhineeth BhatÎncă nu există evaluări
- Lecture 2Document1 paginăLecture 2Abhineeth BhatÎncă nu există evaluări
- Policy For CCC Delayed Start StudentsDocument2 paginiPolicy For CCC Delayed Start StudentsAbhineeth BhatÎncă nu există evaluări
- Lipoprotein Patterns and Associated ConditionsDocument4 paginiLipoprotein Patterns and Associated ConditionsAbhineeth BhatÎncă nu există evaluări
- Wilhelm Endocrine PharmacologyDocument7 paginiWilhelm Endocrine PharmacologyAbhineeth BhatÎncă nu există evaluări
- GuideDocument1 paginăGuideAbhineeth BhatÎncă nu există evaluări
- LabDocument4 paginiLabAbhineeth BhatÎncă nu există evaluări
- Normal Parathyroid GlandsDocument30 paginiNormal Parathyroid GlandsAbhineeth BhatÎncă nu există evaluări
- Question PhilosophyDocument3 paginiQuestion PhilosophyAbhineeth BhatÎncă nu există evaluări
- GuideDocument1 paginăGuideAbhineeth BhatÎncă nu există evaluări
- Aging and MenopauseDocument3 paginiAging and MenopauseAbhineeth BhatÎncă nu există evaluări
- Jefferson - Aoa USMLE Step 1Document12 paginiJefferson - Aoa USMLE Step 1Mc Ase100% (1)
- Lipoprotein Patterns and Associated ConditionsDocument4 paginiLipoprotein Patterns and Associated ConditionsAbhineeth BhatÎncă nu există evaluări
- PancreasDocument8 paginiPancreasAbhineeth BhatÎncă nu există evaluări
- DLL - Science 6 - Q2Document7 paginiDLL - Science 6 - Q2Angelica GuillermoÎncă nu există evaluări
- Paragraph Development ExerciseDocument6 paginiParagraph Development ExerciseSYAFINAS SALAM100% (1)
- The Developing Child - The First Seven Years - EbookDocument141 paginiThe Developing Child - The First Seven Years - Ebookall-natural-nutÎncă nu există evaluări
- Branches of ZoologyDocument3 paginiBranches of ZoologyVivek Morya100% (1)
- Thalassemia: SymptomsDocument3 paginiThalassemia: SymptomsAndi BandotÎncă nu există evaluări
- NCM 100 H.A Procedure DPPER 3Document51 paginiNCM 100 H.A Procedure DPPER 3Richelle Joy Durano RegatunaÎncă nu există evaluări
- Zoology: Zoology Previous Eamcet QuestionsDocument8 paginiZoology: Zoology Previous Eamcet QuestionsGaganpreetSingh100% (1)
- CSIR UGC JRF Subjetive Model Test PaperDocument17 paginiCSIR UGC JRF Subjetive Model Test PaperManu Mallahalli ShanthappaÎncă nu există evaluări
- Point MarmaDocument2 paginiPoint MarmaAnonymous yzbnd8Încă nu există evaluări
- Biology: Revised Syllabus For Higher Secondary First Year CourseDocument4 paginiBiology: Revised Syllabus For Higher Secondary First Year CourseamitumikoibÎncă nu există evaluări
- Supranuclear Control Opf Eye MovementsDocument162 paginiSupranuclear Control Opf Eye Movementsknowledgeguruos179Încă nu există evaluări
- Electrolyte Imbalance 1Document3 paginiElectrolyte Imbalance 1Marius Clifford BilledoÎncă nu există evaluări
- Population Genetics TutorialDocument164 paginiPopulation Genetics TutorialMichelle GÎncă nu există evaluări
- HeparinDocument2 paginiHeparinNinoska Garcia-Ortiz100% (4)
- Pete Pfitzinger Advanced Marathoning Training 88K-1Document8 paginiPete Pfitzinger Advanced Marathoning Training 88K-1Phan ToanÎncă nu există evaluări
- Spesifikasi Patient Monitor: Draeger - Vista 120S: Type Parameter Merk FeaturesDocument3 paginiSpesifikasi Patient Monitor: Draeger - Vista 120S: Type Parameter Merk Featuresflorensia shielyÎncă nu există evaluări
- Tetralogy of Fallot Everything You Wanted To Know But Were Afraid To AskDocument8 paginiTetralogy of Fallot Everything You Wanted To Know But Were Afraid To AsksofiaÎncă nu există evaluări
- Bulacan State University College of Nursing Final Exam ReviewDocument7 paginiBulacan State University College of Nursing Final Exam ReviewDemiar Madlansacay QuintoÎncă nu există evaluări
- Manajemen Pre-Operatif Pasien Dengan DMDocument12 paginiManajemen Pre-Operatif Pasien Dengan DMyanayas28Încă nu există evaluări
- Gavage FeedingDocument18 paginiGavage FeedingMena AmerÎncă nu există evaluări
- Body Systems NotesDocument2 paginiBody Systems NotesAndrea González MercadoÎncă nu există evaluări
- NIOSH Investigation - CR 337 Fire LODDDocument32 paginiNIOSH Investigation - CR 337 Fire LODDRamblingChiefÎncă nu există evaluări
- Musculoskeletal System Lecture NotesDocument169 paginiMusculoskeletal System Lecture Noteszygote0711578796% (28)
- Acute Liver Injury and FailureDocument14 paginiAcute Liver Injury and FailureWeslei ChaconÎncă nu există evaluări
- Chapter 4Document7 paginiChapter 4R LashÎncă nu există evaluări
- Chapter 6 Cell DivisionDocument20 paginiChapter 6 Cell DivisionVinash Shka RaoÎncă nu există evaluări
- Anatomy and Diseases of The UveaDocument102 paginiAnatomy and Diseases of The UveaVishakh IsloorÎncă nu există evaluări
- NCM 103 RLE NOTESDocument8 paginiNCM 103 RLE NOTESgallardo.bettinarose.iÎncă nu există evaluări
- FORENSIC SEROLOGY AND BLOOD ANALYSISDocument16 paginiFORENSIC SEROLOGY AND BLOOD ANALYSISBARCELON, CHRISTOPHER JAMESÎncă nu există evaluări
- Circulatory System: Heart, Blood Vessels & Their FunctionsDocument17 paginiCirculatory System: Heart, Blood Vessels & Their FunctionskangaanushkaÎncă nu există evaluări