S-ar putea să vă placă și
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Form of Charitable Donation Agreement (Non 501 (C) (3) )Document4 paginiForm of Charitable Donation Agreement (Non 501 (C) (3) )maxblauÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Dozier, Sarah V City of Atlanta Et Al - Pacer 112-2Document87 paginiDozier, Sarah V City of Atlanta Et Al - Pacer 112-2maxblauÎncă nu există evaluări
- A Guide To Assett Efficiency OptimizationDocument38 paginiA Guide To Assett Efficiency Optimizationkglorstad100% (1)
- Wakefield, Beasley, and Associates - State Judicial Complex - ProposalDocument50 paginiWakefield, Beasley, and Associates - State Judicial Complex - ProposalmaxblauÎncă nu există evaluări
- Tip-Portfolio AgpaoacirilleDocument130 paginiTip-Portfolio AgpaoacirilleCirille Agpaoa100% (1)
- Stevens & Wilkinson - State Judicial Complex - ProposalDocument50 paginiStevens & Wilkinson - State Judicial Complex - ProposalmaxblauÎncă nu există evaluări
- Pieper O'Brien Herr Architects - State Judicial Complex - ProposalDocument50 paginiPieper O'Brien Herr Architects - State Judicial Complex - ProposalmaxblauÎncă nu există evaluări
- LP in TLE 7 Day 1Document2 paginiLP in TLE 7 Day 1Joseph SuperableÎncă nu există evaluări
- MST121 Course GuideDocument12 paginiMST121 Course Guidejunk6789Încă nu există evaluări
- Dozier, Sarah V City of Atlanta Et Al - Pacer 112-17Document100 paginiDozier, Sarah V City of Atlanta Et Al - Pacer 112-17maxblauÎncă nu există evaluări
- SMMDocument500 paginiSMMbwalya_kakosa561350% (2)
- HOK - State Judicial Complex - ProposalDocument44 paginiHOK - State Judicial Complex - ProposalmaxblauÎncă nu există evaluări
- HRM Report On BeximcoDocument45 paginiHRM Report On BeximcoSadman Shabab Ratul100% (2)
- Lesson 1 Basic Concepts Theories and Principles in Assessing Learning Using Non Traditional MethodsDocument33 paginiLesson 1 Basic Concepts Theories and Principles in Assessing Learning Using Non Traditional MethodsSHSBONI rtu100% (1)
- Stiggins, R. J. (2002) - Assessment Crisis. The Absence of Assessment For Learning. Phi Delta Kappan, 83 (10), 758-765Document8 paginiStiggins, R. J. (2002) - Assessment Crisis. The Absence of Assessment For Learning. Phi Delta Kappan, 83 (10), 758-765Deedee AraaÎncă nu există evaluări
- Missouri, LCME Findings, 2008Document9 paginiMissouri, LCME Findings, 2008maxblauÎncă nu există evaluări
- DOR Brewery ClosingsDocument1 paginăDOR Brewery ClosingsmaxblauÎncă nu există evaluări
- Police Sample Press ReleaseDocument2 paginiPolice Sample Press ReleasemaxblauÎncă nu există evaluări
- Stevens & Wilkinson - Facilities ProgramDocument173 paginiStevens & Wilkinson - Facilities ProgrammaxblauÎncă nu există evaluări
- Dozier, Sarah V City of Atlanta Et Al - Pacer 112-3Document27 paginiDozier, Sarah V City of Atlanta Et Al - Pacer 112-3maxblauÎncă nu există evaluări
- USDOJ DeathRow2013Document22 paginiUSDOJ DeathRow2013maxblauÎncă nu există evaluări
- Missouri, LCME Findings, 2001Document3 paginiMissouri, LCME Findings, 2001maxblauÎncă nu există evaluări
- Dec. 2016 DP ReportDocument38 paginiDec. 2016 DP ReportmaxblauÎncă nu există evaluări
- Dozier, Sarah V City of Atlanta Et Al - Pacer 112-13Document99 paginiDozier, Sarah V City of Atlanta Et Al - Pacer 112-13maxblauÎncă nu există evaluări
- HKS - State Judicial Complex - ProposalDocument38 paginiHKS - State Judicial Complex - ProposalmaxblauÎncă nu există evaluări
- Dozier, Sarah V City of Atlanta Et Al - Pacer 112-4Document27 paginiDozier, Sarah V City of Atlanta Et Al - Pacer 112-4maxblauÎncă nu există evaluări
- Dozier, Sarah V City of Atlanta Et Al - Pacer 112-1Document19 paginiDozier, Sarah V City of Atlanta Et Al - Pacer 112-1maxblauÎncă nu există evaluări
- Georgia Power Energy Capacity MixDocument1 paginăGeorgia Power Energy Capacity MixmaxblauÎncă nu există evaluări
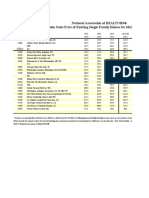
- Metro Home Prices q3 2015 Single Family 2015-11-12Document2 paginiMetro Home Prices q3 2015 Single Family 2015-11-12maxblauÎncă nu există evaluări
- Utility LawsuitDocument27 paginiUtility LawsuitmaxblauÎncă nu există evaluări
- Secretary of State - PeachBreach - Exhibit K - Remedial PoliciesDocument3 paginiSecretary of State - PeachBreach - Exhibit K - Remedial PoliciesmaxblauÎncă nu există evaluări
- Secretary of State - PeachBreach - Exhibit J - Gary Cooley's EmailDocument4.829 paginiSecretary of State - PeachBreach - Exhibit J - Gary Cooley's EmailmaxblauÎncă nu există evaluări
- Secretary of State - PeachBreach - Exhibit I - Gary Cooley's Personnel FileDocument73 paginiSecretary of State - PeachBreach - Exhibit I - Gary Cooley's Personnel FilemaxblauÎncă nu există evaluări
- Secretary of State - PeachBreach - Exhibit H - Documents Related To Voter List RequestsDocument45 paginiSecretary of State - PeachBreach - Exhibit H - Documents Related To Voter List RequestsmaxblauÎncă nu există evaluări
- Secretary of State - PeachBreach - Exhibit G - JIRA TicketsDocument6 paginiSecretary of State - PeachBreach - Exhibit G - JIRA TicketsmaxblauÎncă nu există evaluări
- Secretary of State - PeachBreach - Exhibit E - PCC ReportsDocument3 paginiSecretary of State - PeachBreach - Exhibit E - PCC ReportsmaxblauÎncă nu există evaluări
- Secretary of State - PeachBreach - Exhibit F - Emails Regarding DOR RequestDocument59 paginiSecretary of State - PeachBreach - Exhibit F - Emails Regarding DOR RequestmaxblauÎncă nu există evaluări
- The Implementation of Continuous Assessment in Writing Classes The of Jimma College of Teachers EducationDocument27 paginiThe Implementation of Continuous Assessment in Writing Classes The of Jimma College of Teachers EducationrajaaÎncă nu există evaluări
- Syllabus: Cambridge O Level Environmental ManagementDocument22 paginiSyllabus: Cambridge O Level Environmental Managementmstudy123456Încă nu există evaluări
- BMAN10011 Fundamentals of ManagementDocument3 paginiBMAN10011 Fundamentals of ManagementLukas PedrottaÎncă nu există evaluări
- Albert Diaz-Initial CSTP Self-Assessment-1675328746Document9 paginiAlbert Diaz-Initial CSTP Self-Assessment-1675328746api-668848985Încă nu există evaluări
- Unit Plan Rationale - Abigail GibbonsDocument27 paginiUnit Plan Rationale - Abigail Gibbonsapi-569001953Încă nu există evaluări
- DLL SCIENCE WEEK 10-Fadfwedfwdqgehgda42346532536555seDocument12 paginiDLL SCIENCE WEEK 10-Fadfwedfwdqgehgda42346532536555seDee ZaidÎncă nu există evaluări
- Literacy Progress Units: Writing Organisation - GuidanceDocument18 paginiLiteracy Progress Units: Writing Organisation - GuidanceMatt GrantÎncă nu există evaluări
- Grading System in SyllabusDocument3 paginiGrading System in Syllabusapi-285961875Încă nu există evaluări
- ACC201 - Principles of Accounting - Trimester 1 2021Document10 paginiACC201 - Principles of Accounting - Trimester 1 2021Hoàng Võ Như QuỳnhÎncă nu există evaluări
- Determining Appropriate Physical Education PlacementDocument3 paginiDetermining Appropriate Physical Education PlacementCnu FaiÎncă nu există evaluări
- Mathematics Action PlanDocument5 paginiMathematics Action PlanObong Elementary School (Region VIII - Eastern Samar)Încă nu există evaluări
- Daily Lesson Log - English 9 - Week 2Document5 paginiDaily Lesson Log - English 9 - Week 2Aira Jane CruzÎncă nu există evaluări
- RR 524Document78 paginiRR 524Koshy JohnÎncă nu există evaluări
- MOB75 Engelska Slutprov (Sfi)Document2 paginiMOB75 Engelska Slutprov (Sfi)Mayam AyoÎncă nu există evaluări
- Teaching ESL Learners - Assignment 1 Syllabus Design Tôn N Hoàng Anh Ho Chi Minh City Open UniversityDocument18 paginiTeaching ESL Learners - Assignment 1 Syllabus Design Tôn N Hoàng Anh Ho Chi Minh City Open UniversityAnh TonÎncă nu există evaluări
- SH Choir - March 29Document2 paginiSH Choir - March 29api-299316534Încă nu există evaluări
- Tangram LessonDocument17 paginiTangram Lessondbrizzolara191Încă nu există evaluări
- Curriculum Development & Instructional PlanningDocument2 paginiCurriculum Development & Instructional PlanningJohny VillanuevaÎncă nu există evaluări
- SITXFSA006 Assessment WorkbookDocument55 paginiSITXFSA006 Assessment Workbookindermaan706Încă nu există evaluări
- Barton Reading ProgramDocument7 paginiBarton Reading Programsayer_nicoleÎncă nu există evaluări
- School Excellence Framework (Table)Document1 paginăSchool Excellence Framework (Table)api-290725793Încă nu există evaluări
- EE323 Course Outline 2015 v2Document12 paginiEE323 Course Outline 2015 v2Praneel ChandÎncă nu există evaluări