S-ar putea să vă placă și
- PBL 12 - Adrenal GlandsDocument7 paginiPBL 12 - Adrenal GlandsKrishna OochitÎncă nu există evaluări
- Adrenal Hyperfunction: Cushing'S SyndromeDocument10 paginiAdrenal Hyperfunction: Cushing'S SyndromeJoaquim RodriguezÎncă nu există evaluări
- Dr. Smijal PG Its Year Department of PeriodonticsDocument98 paginiDr. Smijal PG Its Year Department of PeriodonticsMax Fax100% (1)
- ADRENALSDocument60 paginiADRENALSJyoti ChadhaÎncă nu există evaluări
- Darvocet N Drug CardDocument1 paginăDarvocet N Drug CardSheri490Încă nu există evaluări
- WRH Emergency Codes: in Case of Emergency - .Document10 paginiWRH Emergency Codes: in Case of Emergency - .Silvanus Chakra PuspitaÎncă nu există evaluări
- Hand InfectionsDocument41 paginiHand InfectionsUhuebor David50% (2)
- Hand InfectionsDocument41 paginiHand InfectionsUhuebor David50% (2)
- FC Orth (SA) Intermediate Past Papers - 2012 Sept 28-3-2015Document2 paginiFC Orth (SA) Intermediate Past Papers - 2012 Sept 28-3-2015Uhuebor DavidÎncă nu există evaluări
- Bee Empowerment Leslie WilsonDocument6 paginiBee Empowerment Leslie Wilsonchakravartys1327100% (1)
- (Cholinergic System) Model Questions and AnswersDocument45 pagini(Cholinergic System) Model Questions and AnswersAjay SinghÎncă nu există evaluări
- Beta Blockers and Other Sympatholytic AgentsDocument43 paginiBeta Blockers and Other Sympatholytic AgentsAriel OlshevskyÎncă nu există evaluări
- BSS 3rd Edition Participant Handbook CD FinalDocument75 paginiBSS 3rd Edition Participant Handbook CD FinalUhuebor David100% (1)
- Guidelines For The Management of Acute Stroke: Emergency DepartmentDocument10 paginiGuidelines For The Management of Acute Stroke: Emergency DepartmentUhuebor DavidÎncă nu există evaluări
- Endocrine Disorders Cont... (For ADRENAL GLAND)Document4 paginiEndocrine Disorders Cont... (For ADRENAL GLAND)Ernie G. Bautista II, RN, MD100% (3)
- FC Orth (SA) Intermediate Past Papers - 2012 Mar 28-3-2015Document2 paginiFC Orth (SA) Intermediate Past Papers - 2012 Mar 28-3-2015Uhuebor DavidÎncă nu există evaluări
- FC Orth (SA) Intermediate Past Papers - 2012 Mar 28-3-2015Document2 paginiFC Orth (SA) Intermediate Past Papers - 2012 Mar 28-3-2015Uhuebor DavidÎncă nu există evaluări
- Fish Physiology: Fish NeuroendocrinologyDe la EverandFish Physiology: Fish NeuroendocrinologyÎncă nu există evaluări
- Primary Adrenal Insufficiency HandoutDocument2 paginiPrimary Adrenal Insufficiency Handoutapi-614156568Încă nu există evaluări
- Adrenal Gland Final 2Document8 paginiAdrenal Gland Final 2Std DlshsiÎncă nu există evaluări
- 19 SYNTHESIS OF ADRENALINEADRENERGIC RECEPTORS by COL AZMAT ALIDocument53 pagini19 SYNTHESIS OF ADRENALINEADRENERGIC RECEPTORS by COL AZMAT ALIAhmed YTÎncă nu există evaluări
- Adrenocortical Hormones: Learning ObjectivesDocument3 paginiAdrenocortical Hormones: Learning ObjectivesMarlin Berliannanda TawayÎncă nu există evaluări
- Effects Adrenal Hormones RegebDocument7 paginiEffects Adrenal Hormones RegebPraveena MoganÎncă nu există evaluări
- Summary & Mcqs of Adrenal Gland: Done byDocument7 paginiSummary & Mcqs of Adrenal Gland: Done byHabib Ullah100% (1)
- Endocrine System Part 3Document55 paginiEndocrine System Part 3Cristina RocheÎncă nu există evaluări
- Endocrine PhysiologyDocument124 paginiEndocrine PhysiologyEnkusilasie GossaÎncă nu există evaluări
- Adrenal Cortex Disorders NotesDocument3 paginiAdrenal Cortex Disorders NotesGwendareign ElizanÎncă nu există evaluări
- NCMB 316 Lecture & RleDocument34 paginiNCMB 316 Lecture & RleVenansius GanggusÎncă nu există evaluări
- 2021 COMET Krisis Adrenal (Compatibility Mode) (1) - Pages-1-27Document27 pagini2021 COMET Krisis Adrenal (Compatibility Mode) (1) - Pages-1-27Octo IndradjajaÎncă nu există evaluări
- Learning Objectives: Drugs That Enhance Cholinergic TransmissionDocument3 paginiLearning Objectives: Drugs That Enhance Cholinergic TransmissionSamer FarhanÎncă nu există evaluări
- Acute Coronary Syndrome 1Document3 paginiAcute Coronary Syndrome 1Rona PieÎncă nu există evaluări
- (MS II Lec) Endocrine System2Document8 pagini(MS II Lec) Endocrine System2IlawÎncă nu există evaluări
- Ch26 Hormones and The Endocrine SystemDocument13 paginiCh26 Hormones and The Endocrine System鄭心美Încă nu există evaluări
- Adrenal GlandDocument49 paginiAdrenal GlandRaphael AnajeÎncă nu există evaluări
- Pharma Nca1 Notes MidtermDocument8 paginiPharma Nca1 Notes MidtermAICEL A. ABILÎncă nu există evaluări
- VPHM50 Part3 2021Document173 paginiVPHM50 Part3 2021John Joshua J. MingiÎncă nu există evaluări
- Week 11. Endocrinology 3Document17 paginiWeek 11. Endocrinology 3MACOB, ETHELHYN JHANEÎncă nu există evaluări
- 7.endocrine SystemDocument12 pagini7.endocrine SystemElaine Victoria ElizanÎncă nu există evaluări
- AnaesthesiaDocument163 paginiAnaesthesiappp683823Încă nu există evaluări
- Adrenal Gland: The Adrenal Cortex by ZoneDocument9 paginiAdrenal Gland: The Adrenal Cortex by ZoneMiki NishiharaÎncă nu există evaluări
- Chapter 21 Intro To CNS PharmaDocument8 paginiChapter 21 Intro To CNS PharmaChristine Annmarie TapawanÎncă nu există evaluări
- Pharmacodynamics - ReviewerDocument10 paginiPharmacodynamics - ReviewerGabrielle Marie GonzagaÎncă nu există evaluări
- Adrenal GlandDocument2 paginiAdrenal GlandAurelia AlexandraÎncă nu există evaluări
- General Biology Lesson 13Document13 paginiGeneral Biology Lesson 13GUCOR, LOVELY SHANE C.Încă nu există evaluări
- Review of Autonomic PharmacologyDocument42 paginiReview of Autonomic PharmacologyselormniiqÎncă nu există evaluări
- Investigation and Management of Adrenal Disease: The Adrenal Medulla Synthesizes The Catecholamines AdrenalineDocument6 paginiInvestigation and Management of Adrenal Disease: The Adrenal Medulla Synthesizes The Catecholamines AdrenalineMarlin Berliannanda TawayÎncă nu există evaluări
- PHY LE 5 Finals ReviewerDocument26 paginiPHY LE 5 Finals Reviewerroxanne.viriÎncă nu există evaluări
- The Rate Limiting Enzyme The Committed Step: Notes On Enzyme RegulationDocument7 paginiThe Rate Limiting Enzyme The Committed Step: Notes On Enzyme RegulationAkram Khaled Ragab BayoumyÎncă nu există evaluări
- Adrenergic Agonists Lecture 1 - ClarkDocument49 paginiAdrenergic Agonists Lecture 1 - ClarkHaileris1Încă nu există evaluări
- Lecture 10 Steroids (Week 12)Document9 paginiLecture 10 Steroids (Week 12)ahmadslayman1Încă nu există evaluări
- Enzymes in Diagnosis: Prof. Dr. N. Leyla Açan Hacettepe University Faculty of Medicine Department of Medical BiochemistryDocument4 paginiEnzymes in Diagnosis: Prof. Dr. N. Leyla Açan Hacettepe University Faculty of Medicine Department of Medical Biochemistryedh labÎncă nu există evaluări
- ANSDocument42 paginiANSRakshan T100% (1)
- Adrenal Gland: Dr. Fatimah Eliana, SPPD, KemdDocument46 paginiAdrenal Gland: Dr. Fatimah Eliana, SPPD, KemdZahra AstriantaniÎncă nu există evaluări
- LECTURE 6 - Clinical Significance of EnzymesDocument3 paginiLECTURE 6 - Clinical Significance of EnzymesDoreenÎncă nu există evaluări
- Introduction To EndocrinologyDocument8 paginiIntroduction To EndocrinologyAlecx LipatanÎncă nu există evaluări
- Ilovepdf Merged-2Document20 paginiIlovepdf Merged-2Alecx LipatanÎncă nu există evaluări
- Autonomic Drugs 3Document34 paginiAutonomic Drugs 3ismailaiaibrahimÎncă nu există evaluări
- Arterial: An Ncrease in CVP in The Presence ofDocument12 paginiArterial: An Ncrease in CVP in The Presence ofPM Basiloy - AloÎncă nu există evaluări
- HomeostasisDocument34 paginiHomeostasisAwaid AsimÎncă nu există evaluări
- To Convert BUN MG/DL To Urea In, BUN Multiplied With 2.14 - To Convert BUN MG/DL To Urea In, BUN Multiplied With 0.36Document6 paginiTo Convert BUN MG/DL To Urea In, BUN Multiplied With 2.14 - To Convert BUN MG/DL To Urea In, BUN Multiplied With 0.36RALPH JAN T. RIOÎncă nu există evaluări
- Nursing Diagnosis Rationale Intervention Rationale EvaluationDocument3 paginiNursing Diagnosis Rationale Intervention Rationale EvaluationHerald Jones LamirezÎncă nu există evaluări
- ANS Pharmacology DCM 2.1Document115 paginiANS Pharmacology DCM 2.1cyber secÎncă nu există evaluări
- CC2 LecDocument143 paginiCC2 Lechinata shoyoÎncă nu există evaluări
- Future Diagnostic and Therapeutic Targets in CRSDocument163 paginiFuture Diagnostic and Therapeutic Targets in CRSDavid APÎncă nu există evaluări
- Adrenal Gland Cortisol AtfDocument4 paginiAdrenal Gland Cortisol Atf2ymyccmvfcÎncă nu există evaluări
- Acute Coronary SyndromeDocument3 paginiAcute Coronary SyndromeRona PieÎncă nu există evaluări
- Adrenal Cortex DR - GomezDocument13 paginiAdrenal Cortex DR - Gomezvicbart11Încă nu există evaluări
- TOPIC3.4 PHYSIOLOGY Adrenocortical HormonesDocument8 paginiTOPIC3.4 PHYSIOLOGY Adrenocortical HormonesRen AlvÎncă nu există evaluări
- Proteins: M. Zaharna Ckin. Chem. 2009Document28 paginiProteins: M. Zaharna Ckin. Chem. 2009Ahmed GaberÎncă nu există evaluări
- LA Pharma and ArmamentariumDocument59 paginiLA Pharma and ArmamentariumPakistan Dental SocietyÎncă nu există evaluări
- Namastat 118Document56 paginiNamastat 118Uhuebor DavidÎncă nu există evaluări
- Smart GoalsDocument15 paginiSmart GoalsUhuebor DavidÎncă nu există evaluări
- Wound ManagementDocument18 paginiWound ManagementUhuebor DavidÎncă nu există evaluări
- XDR TB NewsDocument1 paginăXDR TB NewsUhuebor DavidÎncă nu există evaluări
- NAMA 7903 Session 1 2018 StudydesignsDocument86 paginiNAMA 7903 Session 1 2018 StudydesignsUhuebor DavidÎncă nu există evaluări
- Purple UrineDocument1 paginăPurple UrineUhuebor DavidÎncă nu există evaluări
- Cardiac MarkersDocument29 paginiCardiac MarkersUhuebor DavidÎncă nu există evaluări
- Introduction To OrthopaedicsDocument53 paginiIntroduction To OrthopaedicsAnn Michelle TarrobagoÎncă nu există evaluări
- Essential Laboratory KnowledgeDocument23 paginiEssential Laboratory KnowledgeUhuebor DavidÎncă nu există evaluări
- August JournalDocument15 paginiAugust JournalUhuebor DavidÎncă nu există evaluări
- Disorders of Carbohydrate Metabolism - HaydenDocument18 paginiDisorders of Carbohydrate Metabolism - HaydenUhuebor DavidÎncă nu există evaluări
- Biochemical Investigation of Renal FunctionDocument34 paginiBiochemical Investigation of Renal FunctionUhuebor DavidÎncă nu există evaluări
- Surgery Orthopedics DR Thurston 2012 - Compressed-3Document139 paginiSurgery Orthopedics DR Thurston 2012 - Compressed-3Uhuebor DavidÎncă nu există evaluări
- Surgery Orthopedics DR Thurston 2012 - Compressed-3Document139 paginiSurgery Orthopedics DR Thurston 2012 - Compressed-3Uhuebor DavidÎncă nu există evaluări
- Orthopaedic EmergenciesDocument12 paginiOrthopaedic EmergenciesUhuebor DavidÎncă nu există evaluări
- (Open) Fractures: Potchefstroom Hopital OrthopedicsDocument9 pagini(Open) Fractures: Potchefstroom Hopital OrthopedicsUhuebor DavidÎncă nu există evaluări
- Abnormalities of The PuepriumDocument14 paginiAbnormalities of The PuepriumUhuebor DavidÎncă nu există evaluări
- VHF Guidelines 5 August 2014Document69 paginiVHF Guidelines 5 August 2014Uhuebor DavidÎncă nu există evaluări
- Local AnaestheticsDocument43 paginiLocal AnaestheticsUhuebor DavidÎncă nu există evaluări
- Crptococcal Meningitis in A Retroviral Positive PatientsDocument18 paginiCrptococcal Meningitis in A Retroviral Positive PatientsUhuebor DavidÎncă nu există evaluări
- Prolonged Pregnancy and Abnormal Fundal HeightDocument15 paginiProlonged Pregnancy and Abnormal Fundal HeightUhuebor DavidÎncă nu există evaluări
- Postmenopausal BleedingDocument29 paginiPostmenopausal BleedingUhuebor DavidÎncă nu există evaluări
- Chapter 10 - Respiratory SystemDocument38 paginiChapter 10 - Respiratory SystemAsma MuhammadÎncă nu există evaluări
- 17.1.19 MRDocument40 pagini17.1.19 MRRosallia MegawatiÎncă nu există evaluări
- CholestyramineDocument1 paginăCholestyramineKatie McPeekÎncă nu există evaluări
- Neurotrac Tens: Operators ManualDocument28 paginiNeurotrac Tens: Operators ManualShane NaidooÎncă nu există evaluări
- Clavicle and Sternoclavicular JointDocument14 paginiClavicle and Sternoclavicular JointChavdarÎncă nu există evaluări
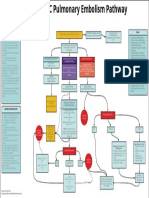
- EMCrit Lae Pulmonary FlowDocument1 paginăEMCrit Lae Pulmonary FlowhmsptrÎncă nu există evaluări
- Biochemistry of Jaundice 03Document52 paginiBiochemistry of Jaundice 03Cathleen May Dela Cruz50% (2)
- Course Task 19Document1 paginăCourse Task 19Laira CañeteÎncă nu există evaluări
- Case Study - 3 - Mumwa Crafts Association - Community Development Through Craft ProductionDocument29 paginiCase Study - 3 - Mumwa Crafts Association - Community Development Through Craft ProductionRifat HasanÎncă nu există evaluări
- 9 Dissacharides Metabolism Compatibility ModeDocument16 pagini9 Dissacharides Metabolism Compatibility ModeAubrey Nativity Ostulano YangzonÎncă nu există evaluări
- Notice: Ocean Transportation Intermediary Licenses: InterCaribbean Cargo, Inc., Et Al.Document2 paginiNotice: Ocean Transportation Intermediary Licenses: InterCaribbean Cargo, Inc., Et Al.Justia.comÎncă nu există evaluări
- HePatic AbscessDocument67 paginiHePatic AbscessCharlie Mignonette BalaÎncă nu există evaluări
- Effectiveness of Workplace Counseling On Employee Performance. A Case of Mumias Sugar Company Limited, KenyaDocument10 paginiEffectiveness of Workplace Counseling On Employee Performance. A Case of Mumias Sugar Company Limited, KenyainventionjournalsÎncă nu există evaluări
- Tromso. Norway Orders Drug-Free Treatment in PsychiatryDocument21 paginiTromso. Norway Orders Drug-Free Treatment in PsychiatryMarcelo Astorga VelosoÎncă nu există evaluări
- This Content Downloaded From 103.251.182.254 On Sat, 18 Jan 2020 04:52:17 UTCDocument9 paginiThis Content Downloaded From 103.251.182.254 On Sat, 18 Jan 2020 04:52:17 UTCsinnanancyÎncă nu există evaluări
- English Grade 4. Unit 6 Healthy World LP 3Document3 paginiEnglish Grade 4. Unit 6 Healthy World LP 3Акниет РахметоваÎncă nu există evaluări
- Human Anatomy & Physiology: Chapter 21-1Document103 paginiHuman Anatomy & Physiology: Chapter 21-1AngelyÎncă nu există evaluări
- Acute PancreatitisDocument9 paginiAcute PancreatitisestefygomezsÎncă nu există evaluări
- Personal Trainer Magazine ISSUE 13Document45 paginiPersonal Trainer Magazine ISSUE 13Jesmin AraÎncă nu există evaluări
- NGS and Sequence Analysis With Biopython For Prospective Brain Cancer Therapeutic StudiesDocument14 paginiNGS and Sequence Analysis With Biopython For Prospective Brain Cancer Therapeutic StudiesIJRASETPublicationsÎncă nu există evaluări
- Murder Mystery 2013Document12 paginiMurder Mystery 2013RAMI FARHATÎncă nu există evaluări
- Evolution in Teddy Grahams MTDocument1 paginăEvolution in Teddy Grahams MTapi-302703920Încă nu există evaluări
- Bowen NeglectDocument46 paginiBowen NeglectwefwfwrÎncă nu există evaluări
- Surgeon's ReportDocument2 paginiSurgeon's ReportjalenÎncă nu există evaluări
- Stacey Luneke ResearchfinalDocument9 paginiStacey Luneke Researchfinalapi-309088550Încă nu există evaluări
- Hiddensee - Michelle HartDocument13 paginiHiddensee - Michelle HartviniciuscarpeÎncă nu există evaluări
- Shingles (Herpes Zoster)Document5 paginiShingles (Herpes Zoster)ceciliafanyÎncă nu există evaluări