S-ar putea să vă placă și
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- APGODocument49 paginiAPGOiamdonutÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Basic Antenatal Care Handbook ISBNDocument59 paginiBasic Antenatal Care Handbook ISBNAuliamusy100% (1)
- MCN PartographDocument2 paginiMCN PartographAlec AnonÎncă nu există evaluări
- Obstetrics & Gynaecology 2019-2008 Regular-Supplementary Group Wise Question Papers WBUHS PDFDocument14 paginiObstetrics & Gynaecology 2019-2008 Regular-Supplementary Group Wise Question Papers WBUHS PDFAditya BarmanÎncă nu există evaluări
- Caesarean SectionDocument48 paginiCaesarean SectionStaen KisÎncă nu există evaluări
- Placenta Previa Case StudyDocument7 paginiPlacenta Previa Case StudyphearlieÎncă nu există evaluări
- Wits Obstetrics 2008Document134 paginiWits Obstetrics 2008Muvenn Kannan100% (1)
- Postpartum QuestionsDocument2 paginiPostpartum QuestionsRayMendez100% (4)
- Placenta: J.L. James, S. Srinivasan, M. Alexander, L.W. ChamleyDocument8 paginiPlacenta: J.L. James, S. Srinivasan, M. Alexander, L.W. ChamleyfujimeisterÎncă nu există evaluări
- Expression of Epithelial Markers by Human Umbilical Cord Stem Cells A Topographical Analysis 2014 PlacentaDocument7 paginiExpression of Epithelial Markers by Human Umbilical Cord Stem Cells A Topographical Analysis 2014 PlacentafujimeisterÎncă nu există evaluări
- In Vitro Transdifferentiation of Umbilical Cord Stem Cells Into Cardiac Myocytes: Role of Growth FactorsDocument8 paginiIn Vitro Transdifferentiation of Umbilical Cord Stem Cells Into Cardiac Myocytes: Role of Growth FactorsfujimeisterÎncă nu există evaluări
- Cord Blood Revelations The Importance of Being A First Born Girl Big On Time and To A Young Mother 2007 Early Human DevelopmentDocument9 paginiCord Blood Revelations The Importance of Being A First Born Girl Big On Time and To A Young Mother 2007 Early Human DevelopmentfujimeisterÎncă nu există evaluări
- European Journal of Obstetrics & Gynecology and Reproductive BiologyDocument7 paginiEuropean Journal of Obstetrics & Gynecology and Reproductive BiologyfujimeisterÎncă nu există evaluări
- Banking Obstetric Related Tissues and Cells What Every Maternity Unit Must Know 2008 Obstetrics Gynaecology Reproductive MedicineDocument4 paginiBanking Obstetric Related Tissues and Cells What Every Maternity Unit Must Know 2008 Obstetrics Gynaecology Reproductive MedicinefujimeisterÎncă nu există evaluări
- Birth Weight As A Risk Factor For Cancer in Adulthood The Stem Cell Perspective 2011 MaturitasDocument3 paginiBirth Weight As A Risk Factor For Cancer in Adulthood The Stem Cell Perspective 2011 MaturitasfujimeisterÎncă nu există evaluări
- Cell Salvage in Obstetrics 2008 International Journal of Obstetric AnesthesiaDocument9 paginiCell Salvage in Obstetrics 2008 International Journal of Obstetric AnesthesiafujimeisterÎncă nu există evaluări
- Poster Session VDocument1 paginăPoster Session VfujimeisterÎncă nu există evaluări
- Effect of Preeclampsia On Umbilical Cord Blood Hematopoietic Progenitor Stem Cells 2001 American Journal of Obstetrics and GynecologyDocument5 paginiEffect of Preeclampsia On Umbilical Cord Blood Hematopoietic Progenitor Stem Cells 2001 American Journal of Obstetrics and GynecologyfujimeisterÎncă nu există evaluări
- Review Endothelial Progenitor Cells in Pregnancy and Obstetric Pathologies 2013 PlacentaDocument6 paginiReview Endothelial Progenitor Cells in Pregnancy and Obstetric Pathologies 2013 PlacentafujimeisterÎncă nu există evaluări
- Stem Cells in Gynecology 2012 American Journal of Obstetrics and GynecologyDocument8 paginiStem Cells in Gynecology 2012 American Journal of Obstetrics and GynecologyfujimeisterÎncă nu există evaluări
- Social Science & Medicine: Julie KentDocument10 paginiSocial Science & Medicine: Julie KentfujimeisterÎncă nu există evaluări
- Impact of Reduced Intensity Conditioning Allogeneic Stem Cell Transplantation On Women S Fertility 2013 Clinical Lymphoma Myeloma and LeukemiaDocument7 paginiImpact of Reduced Intensity Conditioning Allogeneic Stem Cell Transplantation On Women S Fertility 2013 Clinical Lymphoma Myeloma and LeukemiafujimeisterÎncă nu există evaluări
- Optimizing Umbilical Cord Blood Collection Impact of ObstetricDocument3 paginiOptimizing Umbilical Cord Blood Collection Impact of ObstetricGhada AlÎncă nu există evaluări
- Giving To Receive The Right To Donate in Umbilical Cord Blood Banking For Stem Cell Therapies 2012 Health PolicyDocument8 paginiGiving To Receive The Right To Donate in Umbilical Cord Blood Banking For Stem Cell Therapies 2012 Health PolicyfujimeisterÎncă nu există evaluări
- Vitamin D Deficiency Among Adolescent Females With Polycystic Ovary Syndrome 2015 Journal of Pediatric and Adolescent GynecologyDocument4 paginiVitamin D Deficiency Among Adolescent Females With Polycystic Ovary Syndrome 2015 Journal of Pediatric and Adolescent GynecologyfujimeisterÎncă nu există evaluări
- Factors Predicting The Hematopoietic Stem Cells Content of The Umbilical Cord Blood 2013 Transfusion and Apheresis ScienceDocument6 paginiFactors Predicting The Hematopoietic Stem Cells Content of The Umbilical Cord Blood 2013 Transfusion and Apheresis SciencefujimeisterÎncă nu există evaluări
- Utility of The Oral Glucose Tolerance Test To Assess Glucose Abnormalities in Adolescents With Polycystic Ovary Syndrome 2016 Journal of Pediatric andDocument5 paginiUtility of The Oral Glucose Tolerance Test To Assess Glucose Abnormalities in Adolescents With Polycystic Ovary Syndrome 2016 Journal of Pediatric andfujimeisterÎncă nu există evaluări
- Endometriosis - Pathogenesis, Clinical Features, and Diagnosis - UpToDateDocument39 paginiEndometriosis - Pathogenesis, Clinical Features, and Diagnosis - UpToDatefujimeisterÎncă nu există evaluări
- Obstetric Predictors of Placental Umbilical Cord Blood Volume For Transplantation 2003 American Journal of Obstetrics and GynecologyDocument7 paginiObstetric Predictors of Placental Umbilical Cord Blood Volume For Transplantation 2003 American Journal of Obstetrics and GynecologyfujimeisterÎncă nu există evaluări
- Treatment of PCOS in Adolescence 2006 Best Practice Research Clinical Endocrinology MetabolismDocument20 paginiTreatment of PCOS in Adolescence 2006 Best Practice Research Clinical Endocrinology MetabolismfujimeisterÎncă nu există evaluări
- Polycystic Ovary Syndrome An Under Recognized Cause of Abnormal Uterine Bleeding in Adolescents Admitted To A Children S Hospital 2016 Journal of PediDocument7 paginiPolycystic Ovary Syndrome An Under Recognized Cause of Abnormal Uterine Bleeding in Adolescents Admitted To A Children S Hospital 2016 Journal of PedifujimeisterÎncă nu există evaluări
- Utility of Ultrasound in The Diagnosis of Polycystic Ovary Syndrome in Adolescents 2014 Fertility and SterilityDocument7 paginiUtility of Ultrasound in The Diagnosis of Polycystic Ovary Syndrome in Adolescents 2014 Fertility and SterilityfujimeisterÎncă nu există evaluări
- What Is The Risk of Metabolic Syndrome in Adolescents With Normal BMI Who Have Polycystic Ovary Syndrome 2015 Journal of Pediatric and Adolescent GynDocument4 paginiWhat Is The Risk of Metabolic Syndrome in Adolescents With Normal BMI Who Have Polycystic Ovary Syndrome 2015 Journal of Pediatric and Adolescent GynfujimeisterÎncă nu există evaluări
- Whither PCOS The Challenges of Establishing Hyperandrogenism in Adolescent Girls 2008 Journal of Adolescent HealthDocument3 paginiWhither PCOS The Challenges of Establishing Hyperandrogenism in Adolescent Girls 2008 Journal of Adolescent HealthfujimeisterÎncă nu există evaluări
- Polycystic Ovary Syndrome A Review For Dermatologists Part I Diagnosis and Manifestations 2014 Journal of The American Academy of DermatologyDocument10 paginiPolycystic Ovary Syndrome A Review For Dermatologists Part I Diagnosis and Manifestations 2014 Journal of The American Academy of DermatologyfujimeisterÎncă nu există evaluări
- Using The Androgen Excess PCOS Society Criteria To Diagnose Polycystic Ovary Syndrome and The Risk of Metabolic Syndrome in Adolescents 2013 The JournDocument5 paginiUsing The Androgen Excess PCOS Society Criteria To Diagnose Polycystic Ovary Syndrome and The Risk of Metabolic Syndrome in Adolescents 2013 The JournfujimeisterÎncă nu există evaluări
- The Utility of Ultrasonography in The Diagnosis of Polycystic Ovarian Syndrome PCOS in Adolescents 2014 Journal of Pediatric and Adolescent GynecologyDocument1 paginăThe Utility of Ultrasonography in The Diagnosis of Polycystic Ovarian Syndrome PCOS in Adolescents 2014 Journal of Pediatric and Adolescent GynecologyfujimeisterÎncă nu există evaluări
- Conclusions: Background:: Oral Abstracts / J Pediatr Adolesc Gynecol (2013) E47ee53 E49Document2 paginiConclusions: Background:: Oral Abstracts / J Pediatr Adolesc Gynecol (2013) E47ee53 E49fujimeisterÎncă nu există evaluări
- Postnatal Care at The Health Post and in The CommunityDocument23 paginiPostnatal Care at The Health Post and in The CommunityGreggy Francisco LaraÎncă nu există evaluări
- Management of The Third Stage of LaborDocument12 paginiManagement of The Third Stage of Laborayu_pieterÎncă nu există evaluări
- NOTES RLE - Care of Mother, Child at Risk or With Problems (Acute and Chronic)Document2 paginiNOTES RLE - Care of Mother, Child at Risk or With Problems (Acute and Chronic)SteffiÎncă nu există evaluări
- Scaff 1 in SciDocument1 paginăScaff 1 in SciANGEL JASMINE CABADINGÎncă nu există evaluări
- Midwife Skills TrainingDocument3 paginiMidwife Skills TrainingMarjorie Sta. TeresaÎncă nu există evaluări
- Bahasa Inggris Bu YuliDocument8 paginiBahasa Inggris Bu YuliNova FitriaÎncă nu există evaluări
- Bayrampour HamidehDocument267 paginiBayrampour HamidehRohamonangan TheresiaÎncă nu există evaluări
- Pregnancy With Previous LSCS: Vishal Final YearDocument21 paginiPregnancy With Previous LSCS: Vishal Final YearAdit RockÎncă nu există evaluări
- Pengaruh Pijatan Perineum Dan Senam Kegel Terhadap Pengurangan Ruptur Perineum Pada Ibu BersalinDocument7 paginiPengaruh Pijatan Perineum Dan Senam Kegel Terhadap Pengurangan Ruptur Perineum Pada Ibu BersalinPristika wiyarnaÎncă nu există evaluări
- Water BirthDocument17 paginiWater BirthFania PutriÎncă nu există evaluări
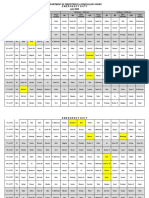
- Department of Obstetrics & Gynecology-Wwrc Emergency Duty July 2020Document3 paginiDepartment of Obstetrics & Gynecology-Wwrc Emergency Duty July 2020noorÎncă nu există evaluări
- 72 Surrogacy CanDocument10 pagini72 Surrogacy CanTamara MoralesÎncă nu există evaluări
- Induction and Augmentation of LaborDocument23 paginiInduction and Augmentation of Laborkevin jonathanÎncă nu există evaluări
- K Rickman ResumeDocument2 paginiK Rickman Resumeapi-286973443Încă nu există evaluări
- CTG Monitoring of Foetal Heart and Uterine ActivityDocument6 paginiCTG Monitoring of Foetal Heart and Uterine ActivityChinedu H. DuruÎncă nu există evaluări
- Uterine Inversion Guide - Causes, Symptoms, TreatmentDocument12 paginiUterine Inversion Guide - Causes, Symptoms, TreatmentElvis NgÎncă nu există evaluări
- Labour Interventions ReportDocument20 paginiLabour Interventions Reportdwi handayaniÎncă nu există evaluări
- 1 - Introduction To MNCHN EINC - 14june2012Document25 pagini1 - Introduction To MNCHN EINC - 14june2012DoyTanÎncă nu există evaluări
- Ahammer Halla Schneeweise JHE 2019Document20 paginiAhammer Halla Schneeweise JHE 2019Grace HallaÎncă nu există evaluări
- Understanding Cephalo-Pelvic Disproportion & Contracted PelvisDocument38 paginiUnderstanding Cephalo-Pelvic Disproportion & Contracted PelvisAltynaiÎncă nu există evaluări
- Soal Bahasa Ingris No 3Document5 paginiSoal Bahasa Ingris No 3Rugas PribawaÎncă nu există evaluări
- Ectopic Pregnancy Diagnosis GuideDocument7 paginiEctopic Pregnancy Diagnosis GuideDr-Saja O. DmourÎncă nu există evaluări