S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
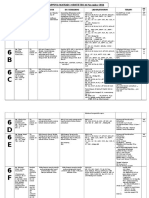
- Mapping Mawar I Obs NOV, 26 2016 Extra RaberDocument3 paginiMapping Mawar I Obs NOV, 26 2016 Extra RaberYohan PamujiÎncă nu există evaluări
- Cover JurnalDocument3 paginiCover JurnalYohan PamujiÎncă nu există evaluări
- Neonatal Morbidity After Maternal Use of Antidepressant Drugs During PregnancyDocument3 paginiNeonatal Morbidity After Maternal Use of Antidepressant Drugs During PregnancyYohan PamujiÎncă nu există evaluări
- Perinato English 14 Nov 2016Document18 paginiPerinato English 14 Nov 2016Yohan PamujiÎncă nu există evaluări
- Via Cryo Training Agenda PATH 2009 rtgutfgirtftg bngfhn hgfh gfhnghn hgn ghn ghngh n dghn dgfn dg nd vhn ghdn gdh ngh n g ng hn dgn g hbn gb ng hn gdhn ghn ghn gd hn gfb fsg dg df fd fg n fghn ghn iugitbhrg fdigod rocihpsrto vcrcjhpordsc pogg vigjh fkgh fdlkgj vklrdg vldrg lrdighlrgkh v vtg vlgh gh vkgjh drghcdsr gcegh cgrcer gDocument4 paginiVia Cryo Training Agenda PATH 2009 rtgutfgirtftg bngfhn hgfh gfhnghn hgn ghn ghngh n dghn dgfn dg nd vhn ghdn gdh ngh n g ng hn dgn g hbn gb ng hn gdhn ghn ghn gd hn gfb fsg dg df fd fg n fghn ghn iugitbhrg fdigod rocihpsrto vcrcjhpordsc pogg vigjh fkgh fdlkgj vklrdg vldrg lrdighlrgkh v vtg vlgh gh vkgjh drghcdsr gcegh cgrcer gYohan PamujiÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Demages Goods RecordDocument22 paginiDemages Goods Recordtariq malikÎncă nu există evaluări
- Neurocisticercosis PDFDocument7 paginiNeurocisticercosis PDFFiorella Alexandra HRÎncă nu există evaluări
- Appendix B - Distance Tables - Metric Units PDFDocument15 paginiAppendix B - Distance Tables - Metric Units PDFitisIÎncă nu există evaluări
- Turning Risk Into ResultsDocument14 paginiTurning Risk Into Resultsririschristin_171952Încă nu există evaluări
- Gendec - Inbound HS-HTNDocument1 paginăGendec - Inbound HS-HTNKhalidÎncă nu există evaluări
- Current Concepts of Enzyme Histochemistry in Modern PathologyDocument11 paginiCurrent Concepts of Enzyme Histochemistry in Modern PathologyRosa AquinoÎncă nu există evaluări
- Data Sheet No. 01.12.01 - PR6 - 7 Inductive Pulse ModuleDocument1 paginăData Sheet No. 01.12.01 - PR6 - 7 Inductive Pulse ModuleThaynar BarbosaÎncă nu există evaluări
- Laboratory Cold ChainDocument22 paginiLaboratory Cold ChainEmiÎncă nu există evaluări
- Congenital Flexural Deformity in CalfDocument6 paginiCongenital Flexural Deformity in CalfBibek SutradharÎncă nu există evaluări
- Study Notes On Isomers and Alkyl HalidesDocument3 paginiStudy Notes On Isomers and Alkyl HalidesChristian Josef AvelinoÎncă nu există evaluări
- Narrative Report On Weekly Accomplishments: Department of EducationDocument2 paginiNarrative Report On Weekly Accomplishments: Department of Educationisha mariano100% (1)
- J130KDocument6 paginiJ130KBelkisa ŠaćiriÎncă nu există evaluări
- GrowNote Faba South 3 Pre PlantingDocument22 paginiGrowNote Faba South 3 Pre PlantingDawitÎncă nu există evaluări
- EIL Document On Motor, PanelDocument62 paginiEIL Document On Motor, PanelArindam Samanta100% (1)
- Health Promotion Officers - CPD Booklet Schedule PDFDocument5 paginiHealth Promotion Officers - CPD Booklet Schedule PDFcharles KadzongaukamaÎncă nu există evaluări
- Drug-Nutrient Interaction in Prescriptions ForDocument7 paginiDrug-Nutrient Interaction in Prescriptions ForRafika DitaÎncă nu există evaluări
- Mycotoxin in Food Supply Chain (Peanuts)Document2 paginiMycotoxin in Food Supply Chain (Peanuts)Ghanthimathi GvsÎncă nu există evaluări
- Mushrooms and Religion: Amanita MuscariaDocument8 paginiMushrooms and Religion: Amanita MuscariaGummyCola50% (2)
- Adenoid HypertrophyDocument56 paginiAdenoid HypertrophyWidi Yuli HariantoÎncă nu există evaluări
- What Is A VolcanoDocument2 paginiWhat Is A VolcanonatachaÎncă nu există evaluări
- As ISO 9919-2004 Pulse Oximeters For Medical Use - RequirementsDocument10 paginiAs ISO 9919-2004 Pulse Oximeters For Medical Use - RequirementsSAI Global - APACÎncă nu există evaluări
- Birding The Gulf Stream: Inside This IssueDocument5 paginiBirding The Gulf Stream: Inside This IssueChoctawhatchee Audubon SocietyÎncă nu există evaluări
- Exercises - Fluid MechanicsDocument3 paginiExercises - Fluid MechanicsgemnikkicÎncă nu există evaluări
- Making Creams With Olive M 1000Document28 paginiMaking Creams With Olive M 1000Nicoleta Chiric0% (1)
- Acute Renal Failure in The Intensive Care Unit: Steven D. Weisbord, M.D., M.Sc. and Paul M. Palevsky, M.DDocument12 paginiAcute Renal Failure in The Intensive Care Unit: Steven D. Weisbord, M.D., M.Sc. and Paul M. Palevsky, M.Dkerm6991Încă nu există evaluări
- Biopolymers: Overview of Several Properties and Consequences On Their ApplicationsDocument10 paginiBiopolymers: Overview of Several Properties and Consequences On Their ApplicationsrafacpereiraÎncă nu există evaluări
- K EtaDocument14 paginiK EtaJosue Teni BeltetonÎncă nu există evaluări
- Eric Koech CV - Docx..bakDocument7 paginiEric Koech CV - Docx..bakPeter Osundwa KitekiÎncă nu există evaluări
- Thanks For Visiting Our Page!: Hi Doc!Document15 paginiThanks For Visiting Our Page!: Hi Doc!bey luÎncă nu există evaluări
- AFMAN91-201 NewDocument458 paginiAFMAN91-201 NewbombtechÎncă nu există evaluări