S-ar putea să vă placă și
- Business English Course BookDocument250 paginiBusiness English Course BookSoodn Kang Soodn100% (5)
- GlaucomaDocument24 paginiGlaucomaSoodn Kang SoodnÎncă nu există evaluări
- Uveal TractDocument11 paginiUveal TractSoodn Kang SoodnÎncă nu există evaluări
- ScleraDocument2 paginiScleraSoodn Kang SoodnÎncă nu există evaluări
- Lacrimal SystemDocument13 paginiLacrimal SystemSoodn Kang SoodnÎncă nu există evaluări
- OrbitDocument9 paginiOrbitSoodn Kang SoodnÎncă nu există evaluări
- RetinaDocument19 paginiRetinaSoodn Kang SoodnÎncă nu există evaluări
- Eyelid 2011Document25 paginiEyelid 2011Soodn Kang SoodnÎncă nu există evaluări
- Pharm DR Ahmed Abd AlrahmanDocument24 paginiPharm DR Ahmed Abd AlrahmanAmrAliTahaÎncă nu există evaluări
- 10 CNS UnlockedDocument51 pagini10 CNS UnlockedSoodn Kang SoodnÎncă nu există evaluări
- Surgery McqsDocument10 paginiSurgery McqsSoodn Kang SoodnÎncă nu există evaluări
- ConjunctivaDocument23 paginiConjunctivaSoodn Kang SoodnÎncă nu există evaluări
- Antidote List 2009: Beaumont Hospital, P.O. BOX 1297, Beaumont Road, Dublin 9Document27 paginiAntidote List 2009: Beaumont Hospital, P.O. BOX 1297, Beaumont Road, Dublin 9Soodn Kang SoodnÎncă nu există evaluări
- AntiarritmiasSzerek 2016-2-8Document30 paginiAntiarritmiasSzerek 2016-2-8Soodn Kang SoodnÎncă nu există evaluări
- Local Anaesthetics Mcqs From LouisDocument2 paginiLocal Anaesthetics Mcqs From LouisSoodn Kang SoodnÎncă nu există evaluări
- Nem-Szteroid Gyulladásgátlók (Nsaids) : 1. Gyulladásgátlás 2. Fájdalomcsillapítás 3. LázcsillapításDocument34 paginiNem-Szteroid Gyulladásgátlók (Nsaids) : 1. Gyulladásgátlás 2. Fájdalomcsillapítás 3. LázcsillapításSoodn Kang SoodnÎncă nu există evaluări
- Pharm Cvs McqsDocument30 paginiPharm Cvs McqsSoodn Kang Soodn100% (3)
- LokalKeringesfokozok B12 Folsav STB ANGOL 2016-2-12Document14 paginiLokalKeringesfokozok B12 Folsav STB ANGOL 2016-2-12Soodn Kang SoodnÎncă nu există evaluări
- Epidemiology of CholeraDocument26 paginiEpidemiology of CholeraSoodn Kang SoodnÎncă nu există evaluări
- Diagnosis 3Document10 paginiDiagnosis 3Soodn Kang SoodnÎncă nu există evaluări
- Hallgatok VeglegesDocument3 paginiHallgatok VeglegesSoodn Kang SoodnÎncă nu există evaluări
- CardiologyDocument10 paginiCardiologySoodn Kang SoodnÎncă nu există evaluări
- DermatologyDocument21 paginiDermatologySoodn Kang SoodnÎncă nu există evaluări
- 2011 - Patient PresentationDocument12 pagini2011 - Patient PresentationSoodn Kang SoodnÎncă nu există evaluări
- Angol Oktatás - VTVSSVTDocument5 paginiAngol Oktatás - VTVSSVTSoodn Kang SoodnÎncă nu există evaluări
- Case Studies in The Management of Acs With GP Iib/Iiia InhibitorsDocument47 paginiCase Studies in The Management of Acs With GP Iib/Iiia InhibitorsSoodn Kang SoodnÎncă nu există evaluări
- Autonomic Drugs Flash CardsDocument16 paginiAutonomic Drugs Flash CardsSoodn Kang SoodnÎncă nu există evaluări
- ورق مذاكره Ent في 100 صفحه بسDocument100 paginiورق مذاكره Ent في 100 صفحه بسSoodn Kang SoodnÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- D. NegligenceDocument11 paginiD. NegligenceKing GeorgeÎncă nu există evaluări
- TOPICS in Health Care ConceptDocument41 paginiTOPICS in Health Care ConcepthageguroÎncă nu există evaluări
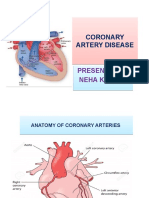
- Coronary Artery DiseaseDocument22 paginiCoronary Artery DiseaseApil BhutaniÎncă nu există evaluări
- Hypokalemic Periodic ParalysisDocument21 paginiHypokalemic Periodic ParalysisVarun VarnÎncă nu există evaluări
- Cardiovascular CirculatoryStudentDocument89 paginiCardiovascular CirculatoryStudentTess MohamedÎncă nu există evaluări
- Exercise Prescription For Health & Fittness For Patients With ObesityDocument1 paginăExercise Prescription For Health & Fittness For Patients With ObesityWasemBhatÎncă nu există evaluări
- Medical-Surgical Nursing Assessment and Management of Clinical Problems 9e Chapter 47Document13 paginiMedical-Surgical Nursing Assessment and Management of Clinical Problems 9e Chapter 47sarasjunkÎncă nu există evaluări
- Management of Primary Dysmenorrhoea by Dry Cupping: A ReviewDocument5 paginiManagement of Primary Dysmenorrhoea by Dry Cupping: A ReviewWilyanto YangÎncă nu există evaluări
- Influenza 1918.0910Document19 paginiInfluenza 1918.0910RafaelÎncă nu există evaluări
- The Right To Health, by Thomas SzaszDocument11 paginiThe Right To Health, by Thomas SzaszNicolas Martin0% (1)
- Vetlexicon News Update - Feb 2020Document2 paginiVetlexicon News Update - Feb 2020TheBoss 20Încă nu există evaluări
- Detailed Lesson Plan BPPDocument8 paginiDetailed Lesson Plan BPPDa Real SoroteÎncă nu există evaluări
- The Mind Into The BodyDocument375 paginiThe Mind Into The BodyΣτάθης Λάζαρης100% (1)
- Case Report DinofilariaDocument4 paginiCase Report DinofilariaKamendra SinghÎncă nu există evaluări
- Example of Nursing Care Plan (Pathophysiology)Document5 paginiExample of Nursing Care Plan (Pathophysiology)Elizabeth ZamoraÎncă nu există evaluări
- Rating The Risk Factors For Breast Cancer: ReviewDocument9 paginiRating The Risk Factors For Breast Cancer: ReviewPratamasari InsaniÎncă nu există evaluări
- Subclinical Thyroid Dysfunction: Diagnosis and Management: Budiman Darmowidjojo, Lucia Dwi AntikaDocument11 paginiSubclinical Thyroid Dysfunction: Diagnosis and Management: Budiman Darmowidjojo, Lucia Dwi AntikaMuhammad Reyhan HidayatÎncă nu există evaluări
- Temperature: Oral, Rectal, Tympanic and Axillary: Using Digital ThermometersDocument4 paginiTemperature: Oral, Rectal, Tympanic and Axillary: Using Digital ThermometersStephanie LopezÎncă nu există evaluări
- TERMINOLOGI 2 ST - PencernaanDocument61 paginiTERMINOLOGI 2 ST - PencernaanSarah Suzanna Sitepu0% (1)
- Chest Trauma DikaDocument46 paginiChest Trauma DikaOnyedika EgbujoÎncă nu există evaluări
- The Only Way To Achieve Harmony Is Through Practicing MindfulnessDocument8 paginiThe Only Way To Achieve Harmony Is Through Practicing MindfulnessAnn ZhyhalkinaÎncă nu există evaluări
- Advanced Writing SkillsDocument74 paginiAdvanced Writing SkillsThaiHoa9100% (1)
- Proceeding 4th Aceh Surgery UpdateDocument83 paginiProceeding 4th Aceh Surgery UpdateUNS KAMERA BELAKANGÎncă nu există evaluări
- FAD DIETS PowerPointDocument48 paginiFAD DIETS PowerPointTechnoShindoÎncă nu există evaluări
- NANDA LIST of N.DiagnosesDocument3 paginiNANDA LIST of N.DiagnosesHasan KasiÎncă nu există evaluări
- Subiecte Oral Engleza BilingvDocument3 paginiSubiecte Oral Engleza BilingvRadu Bortes100% (1)
- MCQ Ped EndocvsDocument2 paginiMCQ Ped EndocvsManveerÎncă nu există evaluări
- Anesthesia MCQ 425Document4 paginiAnesthesia MCQ 425dungulu50% (2)
- Practice Essentials: Essential Updates: Distinguishing Between Left-And Right-Sided Atrial TachycardiaDocument28 paginiPractice Essentials: Essential Updates: Distinguishing Between Left-And Right-Sided Atrial TachycardiaRully SyahrizalÎncă nu există evaluări
- Princess Diana SpeechDocument5 paginiPrincess Diana SpeechPasca AlexÎncă nu există evaluări