S-ar putea să vă placă și
- Diagnostic Neuroradiology: A Practical Guide and CasesDe la EverandDiagnostic Neuroradiology: A Practical Guide and CasesÎncă nu există evaluări
- Point of Care Ultrasound: The Critical Imaging Tool For The Critically UnwellDocument10 paginiPoint of Care Ultrasound: The Critical Imaging Tool For The Critically UnwellOswaldo OrtizÎncă nu există evaluări
- Conlon 2019 JJJJJDocument19 paginiConlon 2019 JJJJJDr.gendjutÎncă nu există evaluări
- 1.1. Pocus en Emg y Critical Care 2018 PDFDocument8 pagini1.1. Pocus en Emg y Critical Care 2018 PDFEmergencias RebagliatiÎncă nu există evaluări
- Point of Care Ultrasound For The ClinicalDocument14 paginiPoint of Care Ultrasound For The Clinical凌晓敏Încă nu există evaluări
- Point-of-Care Ultrasonography For Primary Care PhyDocument18 paginiPoint-of-Care Ultrasonography For Primary Care PhyFrederico PóvoaÎncă nu există evaluări
- Recommendations For The Use of Point-Of-Care Ultrasound (POCUS) by Emergency Physicians in CanadaDocument6 paginiRecommendations For The Use of Point-Of-Care Ultrasound (POCUS) by Emergency Physicians in CanadaandresÎncă nu există evaluări
- POCUS Point of Care Ultrasound AdvancedDocument1 paginăPOCUS Point of Care Ultrasound Advancedahmet kutluayÎncă nu există evaluări
- POCUS NEJM ArticleDocument10 paginiPOCUS NEJM ArticleSrishti GoenkaÎncă nu există evaluări
- Nejmra 1916062Document10 paginiNejmra 1916062Sebastian Medina RiveraÎncă nu există evaluări
- NEJM 2021 - Point-of-Care UltrasonographyDocument10 paginiNEJM 2021 - Point-of-Care UltrasonographylagianggenÎncă nu există evaluări
- Bedside POCUS During Ward Emergencies Is Associated With Improved Diagnosis and Outcome: An Observational, Prospective, Controlled StudyDocument12 paginiBedside POCUS During Ward Emergencies Is Associated With Improved Diagnosis and Outcome: An Observational, Prospective, Controlled StudyADRIANA FERNANDA MENESES AYALAÎncă nu există evaluări
- Point of Care Ultrasound Potential and LimitationsDocument3 paginiPoint of Care Ultrasound Potential and Limitationsjorge.vicencioÎncă nu există evaluări
- Semana 1-Paper, Fundamentals of US in Clinical PracticeDocument14 paginiSemana 1-Paper, Fundamentals of US in Clinical PracticeRudy AravenaÎncă nu există evaluări
- Marbach Et Al.Document12 paginiMarbach Et Al.lfei1216Încă nu există evaluări
- POCUS1Document18 paginiPOCUS1AME BAHIAÎncă nu există evaluări
- POCUSDocument10 paginiPOCUSSMIBA MedicinaÎncă nu există evaluări
- ACEP Emergency US GuidelinesDocument38 paginiACEP Emergency US GuidelinespegehringÎncă nu există evaluări
- The Ultrasound PractitionerDocument32 paginiThe Ultrasound PractitionerWebster The-TechGuy Lungu100% (1)
- RMI 40095 Impact of Point of Care Ultrasound On Quality of Care in Cli 090514Document13 paginiRMI 40095 Impact of Point of Care Ultrasound On Quality of Care in Cli 090514Ahmedaref EzrinÎncă nu există evaluări
- Presentation 2Document1 paginăPresentation 2jmasiak67Încă nu există evaluări
- Curriculum For Fundamentals of Ultrasound in Clinical PracticeDocument15 paginiCurriculum For Fundamentals of Ultrasound in Clinical PracticeLAURA SOFIA PASTRANA CORTESÎncă nu există evaluări
- Development of A Modified Swallowing Screening TooDocument7 paginiDevelopment of A Modified Swallowing Screening TooNADISH MANZOORÎncă nu există evaluări
- Díaz Gómez José L Point of Care Ultrasonography 2021Document10 paginiDíaz Gómez José L Point of Care Ultrasonography 2021cristianÎncă nu există evaluări
- Ketelaars2018 Article ABCDEOfPrehospitalUltrasonograDocument18 paginiKetelaars2018 Article ABCDEOfPrehospitalUltrasonograPedito PicapiedraÎncă nu există evaluări
- Special Article: Correspondence ToDocument34 paginiSpecial Article: Correspondence TodrsubramanianÎncă nu există evaluări
- Radiology For Maxillofacial Surgeons The EssentialDocument49 paginiRadiology For Maxillofacial Surgeons The EssentialAbdulkadir AwadhÎncă nu există evaluări
- Ultrasonographic-Guided Resuscitation of The Surgical PatientDocument2 paginiUltrasonographic-Guided Resuscitation of The Surgical PatientAndreia MattiuciÎncă nu există evaluări
- USG For Critical Care PDFDocument13 paginiUSG For Critical Care PDFachyutsharmaÎncă nu există evaluări
- Proactive Medicine: The "UCI 30," An Ultrasound-Based Clinical Initiative From The University of California, IrvineDocument6 paginiProactive Medicine: The "UCI 30," An Ultrasound-Based Clinical Initiative From The University of California, Irvineelectron_glowÎncă nu există evaluări
- POCUS in Nephrology Overview Rationale For Use and ScopeDocument7 paginiPOCUS in Nephrology Overview Rationale For Use and ScopekingbavaÎncă nu există evaluări
- An Overview of Emergency Ultrasound in The United States: Jeremy A. MichalkeDocument6 paginiAn Overview of Emergency Ultrasound in The United States: Jeremy A. Michalkeratih kumalasariÎncă nu există evaluări
- 2008 Ultrasound Guidelines ACEPDocument42 pagini2008 Ultrasound Guidelines ACEPlevinson9112860Încă nu există evaluări
- An Overview of Emergency Ultrasound in The United StatesDocument6 paginiAn Overview of Emergency Ultrasound in The United StatesNuriakhildaÎncă nu există evaluări
- POCUS 25 Practice DomainsDocument8 paginiPOCUS 25 Practice DomainsrajkumarrajendramÎncă nu există evaluări
- Point of Care Ultrasound With Pocket Size Devices in Emergency Department - 2019Document10 paginiPoint of Care Ultrasound With Pocket Size Devices in Emergency Department - 2019ntnquynhproÎncă nu există evaluări
- Orhan 2021 (Book) - Ultrasonography in Dentomaxillofacial Diagnostics - SpringerDocument372 paginiOrhan 2021 (Book) - Ultrasonography in Dentomaxillofacial Diagnostics - SpringerlagianggenÎncă nu există evaluări
- Bedside Emergency Cardiac Ultrasound in ChildrenDocument11 paginiBedside Emergency Cardiac Ultrasound in ChildrenNikhil KumarÎncă nu există evaluări
- Ultrasound in Gynecology and ObstetricsDocument197 paginiUltrasound in Gynecology and ObstetricsAli Murtaza AbbasÎncă nu există evaluări
- Lung Ultrasound For Critical Care PhysiotherapistsDocument8 paginiLung Ultrasound For Critical Care PhysiotherapistsArturo Loyola MaturanaÎncă nu există evaluări
- HSR2 5 E649Document9 paginiHSR2 5 E649Samsul BahriÎncă nu există evaluări
- 1 5136382648058380752Document11 pagini1 5136382648058380752ednasu1Încă nu există evaluări
- Why Anesthesiologists Must Incorporate Focused Cardiac Ultrasound Into Daily PracticeDocument5 paginiWhy Anesthesiologists Must Incorporate Focused Cardiac Ultrasound Into Daily PracticePaola CastellanosÎncă nu există evaluări
- Point-of-Care Ultrasound: Not A Stethoscope-A Separate Clinical EntityDocument2 paginiPoint-of-Care Ultrasound: Not A Stethoscope-A Separate Clinical Entityapi-274764147Încă nu există evaluări
- POCUSenColelitiasis 200618 162923Document5 paginiPOCUSenColelitiasis 200618 162923David Salomon Gomez AscencioÎncă nu există evaluări
- Ultrasonographic Examination of The Equine Neonate Thorax and AbdomenDocument29 paginiUltrasonographic Examination of The Equine Neonate Thorax and Abdomenludiegues752Încă nu există evaluări
- Lung Ultrasound-The Emerging Role of Respiratory TherapistsDocument13 paginiLung Ultrasound-The Emerging Role of Respiratory TherapistsArturo Loyola MaturanaÎncă nu există evaluări
- 2009 Article 7 PDFDocument10 pagini2009 Article 7 PDFJesse CusterÎncă nu există evaluări
- Laura C Scholtz Ultrasonography in Neurology ADocument10 paginiLaura C Scholtz Ultrasonography in Neurology AJuliaÎncă nu există evaluări
- Research Open Access: Singh Et Al. Critical Care (2020) 24:65Document16 paginiResearch Open Access: Singh Et Al. Critical Care (2020) 24:65BrîndușaPetcariuÎncă nu există evaluări
- Role of Diagnostic Point-Of-Care Ultrasound in Preoperative Optimization: A Narrative ReviewDocument5 paginiRole of Diagnostic Point-Of-Care Ultrasound in Preoperative Optimization: A Narrative ReviewdrsubramanianÎncă nu există evaluări
- CJASN POCUS EditorialDocument4 paginiCJASN POCUS EditorialkingbavaÎncă nu există evaluări
- The European Society of Gynaecological Oncology:European Society For Radiotherapy and Oncology:European Society of Pathology Guidelines For The Management of Patients With Cervical CancerDocument18 paginiThe European Society of Gynaecological Oncology:European Society For Radiotherapy and Oncology:European Society of Pathology Guidelines For The Management of Patients With Cervical CancerKaleb Rudy HartawanÎncă nu există evaluări
- Echocardiography in ShockDocument7 paginiEchocardiography in ShockRaul ForjanÎncă nu există evaluări
- Cureus 0010 00000002076Document7 paginiCureus 0010 00000002076resmi suciÎncă nu există evaluări
- Point-Of-Care Gastric Ultrasound and Aspiration Risk Assessment - A Narrative Review PDFDocument12 paginiPoint-Of-Care Gastric Ultrasound and Aspiration Risk Assessment - A Narrative Review PDFJohana FuentesÎncă nu există evaluări
- Indications For Bedside Ultrasonography in The Critically-Ill Adult Patient - UpToDate (Completo)Document31 paginiIndications For Bedside Ultrasonography in The Critically-Ill Adult Patient - UpToDate (Completo)Giulio MilanezÎncă nu există evaluări
- The Pathophysiologic Basis of Nuclear MedicineDocument21 paginiThe Pathophysiologic Basis of Nuclear MedicineShazia FatimaÎncă nu există evaluări
- Fuile 4Document19 paginiFuile 4Paulo RosÎncă nu există evaluări
- Cardiopulmonary Point of Care Ultrasound (2023)Document388 paginiCardiopulmonary Point of Care Ultrasound (2023)xf5tsxrgypÎncă nu există evaluări
- Paediatric Surgery For Congenital Anomalies The Next Frontier - 2021 - The LanDocument2 paginiPaediatric Surgery For Congenital Anomalies The Next Frontier - 2021 - The LanAvril JatariuÎncă nu există evaluări
- Anatomy and Physiology of The Nose and Paranasal Sinuses. Diagnosis and Management of RhinosinusitisDocument87 paginiAnatomy and Physiology of The Nose and Paranasal Sinuses. Diagnosis and Management of RhinosinusitisDanielicah Cruz100% (1)
- Indraprasthaapollo Hospital, New Delhi: Antony T RaphelDocument12 paginiIndraprasthaapollo Hospital, New Delhi: Antony T Raphelantony t raphel0% (1)
- Esophageal Atresia History, Embryology, ClassificationDocument21 paginiEsophageal Atresia History, Embryology, ClassificationOktania Putri Kusnawan100% (2)
- Anticoagulation Reversal AgentsDocument3 paginiAnticoagulation Reversal AgentsElaine Yves JulineÎncă nu există evaluări
- Apical Extrusion of Debris and Irrigant Using HandDocument25 paginiApical Extrusion of Debris and Irrigant Using HandManva MonishÎncă nu există evaluări
- Topical Atropine Mydriasis RabbitDocument3 paginiTopical Atropine Mydriasis RabbitPadmanabha Gowda100% (1)
- CPR and First Aid PowerpointDocument21 paginiCPR and First Aid PowerpointZawawiIbnuRosyidÎncă nu există evaluări
- Thyroid Ultrasound For Thyroidologists: Durr-e-SabihDocument49 paginiThyroid Ultrasound For Thyroidologists: Durr-e-SabihMakmun RadÎncă nu există evaluări
- Cruise Ship Health Care Guidelines PrepDocument8 paginiCruise Ship Health Care Guidelines PrepMaxMusterÎncă nu există evaluări
- ADEA CAAPID InstructionsDocument10 paginiADEA CAAPID Instructionsshyam05_narainÎncă nu există evaluări
- Basketball InjuriesDocument2 paginiBasketball Injuriesapi-335139173Încă nu există evaluări
- Reading ListDocument4 paginiReading Listmehmoodabid84Încă nu există evaluări
- Selected Bibliography On DreamingDocument29 paginiSelected Bibliography On DreamingkayarÎncă nu există evaluări
- Uss Features of Iugr and Macrosomia.Document11 paginiUss Features of Iugr and Macrosomia.ibmreadywriterÎncă nu există evaluări
- Management of Children With Autism Spectrum Disorders: PediatricsDocument23 paginiManagement of Children With Autism Spectrum Disorders: Pediatricspidal_jose89Încă nu există evaluări
- Baba Farid University of Health Sciences, Sadiq Road, Faridkot Ph. 01639-256232, 256236 Advt. No 06/2020 VacanciesDocument4 paginiBaba Farid University of Health Sciences, Sadiq Road, Faridkot Ph. 01639-256232, 256236 Advt. No 06/2020 VacanciesSinghTarunÎncă nu există evaluări
- Administering Intramuscular Injections To Children - What Does The Evidence Say?Document8 paginiAdministering Intramuscular Injections To Children - What Does The Evidence Say?ZACHARIAH MANKIRÎncă nu există evaluări
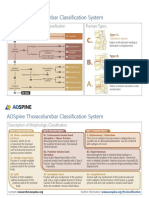
- AOSpine Thoracolumbar Classification System - Pocket CardDocument2 paginiAOSpine Thoracolumbar Classification System - Pocket CardFernanda Ahumada0% (1)
- Ankylosing Spondylitis and HomoeopathyDocument12 paginiAnkylosing Spondylitis and HomoeopathyDr. Rajneesh Kumar Sharma MD HomÎncă nu există evaluări
- Plagiocefalia PDFDocument10 paginiPlagiocefalia PDFIlwen LlanquilefÎncă nu există evaluări
- Vertigo DavidsonDocument13 paginiVertigo DavidsonifahInayahÎncă nu există evaluări
- CV DR IhabDocument4 paginiCV DR IhabIhab SulimanÎncă nu există evaluări
- CRT BacteriaDocument15 paginiCRT BacteriatsntiÎncă nu există evaluări
- Core Topics in Internal MedicineDocument4 paginiCore Topics in Internal MedicineKristina Anne CoÎncă nu există evaluări
- Raja Rajeshwari Medical CollegeDocument11 paginiRaja Rajeshwari Medical CollegepentagoneducationÎncă nu există evaluări
- Canadian Guidelines 2018Document6 paginiCanadian Guidelines 2018Eduardo JiménezÎncă nu există evaluări
- Provider Manual Part 2 Attachments and Forms - 082013Document74 paginiProvider Manual Part 2 Attachments and Forms - 082013Tuyet-Lan BuiÎncă nu există evaluări
- Stretching With Children With Cerebral Palsy What.8 PDFDocument6 paginiStretching With Children With Cerebral Palsy What.8 PDFNurul FadhillahÎncă nu există evaluări
- HOSPITAL Literature Study and Case StudyDocument63 paginiHOSPITAL Literature Study and Case StudyAvantikaÎncă nu există evaluări
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDe la EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionEvaluare: 4 din 5 stele4/5 (402)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessDe la EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessEvaluare: 4.5 din 5 stele4.5/5 (327)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDe la EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityEvaluare: 4 din 5 stele4/5 (13)
- The Ultimate Guide To Memory Improvement TechniquesDe la EverandThe Ultimate Guide To Memory Improvement TechniquesEvaluare: 5 din 5 stele5/5 (34)
- Techniques Exercises And Tricks For Memory ImprovementDe la EverandTechniques Exercises And Tricks For Memory ImprovementEvaluare: 4.5 din 5 stele4.5/5 (40)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDe la EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsEvaluare: 3.5 din 5 stele3.5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDe la EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeÎncă nu există evaluări
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDe la EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedEvaluare: 5 din 5 stele5/5 (78)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisDe la EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisEvaluare: 4 din 5 stele4/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDe la EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityEvaluare: 3.5 din 5 stele3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDe la EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsÎncă nu există evaluări
- The Obesity Code: Unlocking the Secrets of Weight LossDe la EverandThe Obesity Code: Unlocking the Secrets of Weight LossEvaluare: 5 din 5 stele5/5 (3)
- The Happiness Trap: How to Stop Struggling and Start LivingDe la EverandThe Happiness Trap: How to Stop Struggling and Start LivingEvaluare: 4 din 5 stele4/5 (1)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingDe la EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingEvaluare: 5 din 5 stele5/5 (4)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingDe la EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingEvaluare: 3.5 din 5 stele3.5/5 (32)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDe la EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsEvaluare: 4.5 din 5 stele4.5/5 (169)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDe la EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsDe la EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsÎncă nu există evaluări
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDe la EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisEvaluare: 4.5 din 5 stele4.5/5 (41)
- The Tennis Partner: A Doctor's Story of Friendship and LossDe la EverandThe Tennis Partner: A Doctor's Story of Friendship and LossEvaluare: 4.5 din 5 stele4.5/5 (4)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisDe la EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisEvaluare: 5 din 5 stele5/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.De la EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Evaluare: 4.5 din 5 stele4.5/5 (110)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisDe la EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisEvaluare: 5 din 5 stele5/5 (8)