S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Sop-001 Cleaning-Procedure-WarehouseDocument6 paginiSop-001 Cleaning-Procedure-WarehouseAheed Khokhar100% (4)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Fetal Pharmacotherapy PDFDocument17 paginiFetal Pharmacotherapy PDFPrasanna BabuÎncă nu există evaluări
- IndianJPharmacol493229-3498174 094301Document7 paginiIndianJPharmacol493229-3498174 094301Prasanna BabuÎncă nu există evaluări
- Carbohydrates and Drug Design PDFDocument24 paginiCarbohydrates and Drug Design PDFPrasanna BabuÎncă nu există evaluări
- Metabolism-Based Drug Design and Drug Ta PDFDocument6 paginiMetabolism-Based Drug Design and Drug Ta PDFPrasanna BabuÎncă nu există evaluări
- Homeopathy and PlaceboDocument2 paginiHomeopathy and PlaceboPrasanna BabuÎncă nu există evaluări
- Ethnopharmacological Aspects of Resverat PDFDocument6 paginiEthnopharmacological Aspects of Resverat PDFPrasanna BabuÎncă nu există evaluări
- Antiglaucoma PharmacotherapyDocument5 paginiAntiglaucoma PharmacotherapyPrasanna BabuÎncă nu există evaluări
- Coronary Adjunctive PharmacotherapyDocument6 paginiCoronary Adjunctive PharmacotherapyPrasanna BabuÎncă nu există evaluări
- Novel Strategies of Aerosolic PharmacothDocument5 paginiNovel Strategies of Aerosolic PharmacothPrasanna BabuÎncă nu există evaluări
- Introduction Emergency Medicine PharmacoDocument2 paginiIntroduction Emergency Medicine PharmacoPrasanna BabuÎncă nu există evaluări
- Pharmacotherapy For Premature EjaculatioDocument11 paginiPharmacotherapy For Premature EjaculatioPrasanna BabuÎncă nu există evaluări
- Depilatory HerbalDocument10 paginiDepilatory HerbalAbdul SattarÎncă nu există evaluări
- Pharmacotherapy of Eating Disorders PDFDocument20 paginiPharmacotherapy of Eating Disorders PDFPrasanna BabuÎncă nu există evaluări
- Pharmacotherapy For Erectile DysfunctionDocument64 paginiPharmacotherapy For Erectile DysfunctionPrasanna BabuÎncă nu există evaluări
- Tmp5a93 TMPDocument4 paginiTmp5a93 TMPFrontiersÎncă nu există evaluări
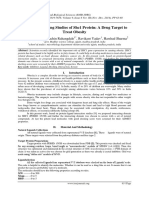
- Molecular Docking Studies of Shc1 Protein: A Drug Target To Treat ObesityDocument6 paginiMolecular Docking Studies of Shc1 Protein: A Drug Target To Treat ObesityPrasanna BabuÎncă nu există evaluări
- Integrative Oncotherapy - Lessons From Ou PDFDocument1 paginăIntegrative Oncotherapy - Lessons From Ou PDFPrasanna BabuÎncă nu există evaluări
- Ayurveda A Multilectic InterpretationDocument8 paginiAyurveda A Multilectic InterpretationPrasanna BabuÎncă nu există evaluări
- A Machine Learning-Based Method To Impro PDFDocument27 paginiA Machine Learning-Based Method To Impro PDFPrasanna BabuÎncă nu există evaluări
- Homeopathic PharmacyDocument376 paginiHomeopathic PharmacyBlitzone100% (12)
- Comparative Docking Studies On ErlotinibDocument7 paginiComparative Docking Studies On ErlotinibPrasanna BabuÎncă nu există evaluări
- Structure-Based Drug Design Docking and PDFDocument18 paginiStructure-Based Drug Design Docking and PDFPrasanna BabuÎncă nu există evaluări
- Molecular Docking Studies of Shc1 Protein: A Drug Target To Treat ObesityDocument6 paginiMolecular Docking Studies of Shc1 Protein: A Drug Target To Treat ObesityPrasanna BabuÎncă nu există evaluări
- Noble Metal Nanoparticles Applications I PDFDocument13 paginiNoble Metal Nanoparticles Applications I PDFPrasanna BabuÎncă nu există evaluări
- Detal PasteDocument8 paginiDetal PastePrasanna BabuÎncă nu există evaluări
- Current Advances in Transdermal Delivery of Drugs For Alzheimer's DiseaseDocument10 paginiCurrent Advances in Transdermal Delivery of Drugs For Alzheimer's DiseasePrasanna BabuÎncă nu există evaluări
- 1Document6 pagini1Prasanna BabuÎncă nu există evaluări
- Research Paper: Indian J Pharmacol April 2005 Vol 37 Issue 2 103-110Document8 paginiResearch Paper: Indian J Pharmacol April 2005 Vol 37 Issue 2 103-110Prasanna BabuÎncă nu există evaluări
- 4Document5 pagini4Prasanna BabuÎncă nu există evaluări
- Anonciata Murigo Nurse Counselor Resume 2021Document2 paginiAnonciata Murigo Nurse Counselor Resume 2021Mai TapiwaÎncă nu există evaluări
- Single Modified Ilioinguinal Approach For The Treatment of Acetabular Fractures Involving Both ColumnsDocument8 paginiSingle Modified Ilioinguinal Approach For The Treatment of Acetabular Fractures Involving Both ColumnsamineÎncă nu există evaluări
- Surgical DressingDocument7 paginiSurgical DressingGabz GabbyÎncă nu există evaluări
- Stress: Hans Selye's Model of StressDocument3 paginiStress: Hans Selye's Model of StressSiddharth VermaÎncă nu există evaluări
- Health and Safety Legislation and Regulations PowerpointDocument21 paginiHealth and Safety Legislation and Regulations PowerpointmichelleÎncă nu există evaluări
- CHN1 Lec Session #14 SASDocument6 paginiCHN1 Lec Session #14 SASJhanna Mae BalbonÎncă nu există evaluări
- SeminarDocument6 paginiSeminarDoktere WongndesoÎncă nu există evaluări
- Vampire, Wraith - Necromancy ReduxDocument6 paginiVampire, Wraith - Necromancy ReduxDDTWilsonÎncă nu există evaluări
- Viva Q-Ans Class XiiDocument10 paginiViva Q-Ans Class Xiipavani pavakiÎncă nu există evaluări
- Goodman, Ashley SignedDocument1 paginăGoodman, Ashley SignedAshley GoodmanÎncă nu există evaluări
- FNCPDocument11 paginiFNCPCATHRYN MAE GAYLANÎncă nu există evaluări
- BGS Interim ReportDocument8 paginiBGS Interim ReportGaurav KishoreÎncă nu există evaluări
- 2o Tarol, RichelleDocument1 pagină2o Tarol, Richelleangelo hijalgaÎncă nu există evaluări
- Contaminacion y FN Pulmonar en NiñosDocument14 paginiContaminacion y FN Pulmonar en NiñosLaura del pinoÎncă nu există evaluări
- PTS I Bhs Inggris XIIDocument7 paginiPTS I Bhs Inggris XIIVriska Budi pratiwiÎncă nu există evaluări
- ELG-2 Datalogger Wireless Telemetry For Mouse & Rat Amuza IncDocument21 paginiELG-2 Datalogger Wireless Telemetry For Mouse & Rat Amuza IncGeneration GenerationÎncă nu există evaluări
- Spirituality Among Retired PersonsDocument4 paginiSpirituality Among Retired PersonsEditor IJTSRDÎncă nu există evaluări
- SSC CGL Mains 2023 (4 Mock Test)Document23 paginiSSC CGL Mains 2023 (4 Mock Test)M thebluegirlÎncă nu există evaluări
- Optic Disc CuppingDocument14 paginiOptic Disc CuppingAsri Kartika AnggraeniÎncă nu există evaluări
- Tutorial 6Document6 paginiTutorial 6guddu guptaÎncă nu există evaluări
- Lakewood Police Department Return To Work Decision MatrixDocument1 paginăLakewood Police Department Return To Work Decision MatrixMichael_Roberts2019Încă nu există evaluări
- Re-Registration Form DNCDocument2 paginiRe-Registration Form DNCSeema KhuranaÎncă nu există evaluări
- Soal News ItemDocument11 paginiSoal News ItemYehezkiel Rivaldo Widjaya100% (1)
- MAPEH (P.E.) : Quarter 2 - Module1Document24 paginiMAPEH (P.E.) : Quarter 2 - Module1EloizaÎncă nu există evaluări
- Lesson PlanDocument3 paginiLesson PlanJOSHUA ESTRADAÎncă nu există evaluări
- 23a5152 237332Document24 pagini23a5152 237332Mohammed. AbdiÎncă nu există evaluări
- Physiological Psychology - Critique PaperDocument2 paginiPhysiological Psychology - Critique PaperJoan Marie LucenaÎncă nu există evaluări
- How To Dominate The Ventilator: Spinning DialsDocument5 paginiHow To Dominate The Ventilator: Spinning DialsIgnacia Cid PintoÎncă nu există evaluări
- 4 Risk Management ProcessDocument35 pagini4 Risk Management Processfrancis malamaÎncă nu există evaluări