S-ar putea să vă placă și
- Border Collie Training GuidelinesDocument12 paginiBorder Collie Training GuidelinespsmanasseÎncă nu există evaluări
- Chemical Engineering Projects List For Final YearDocument2 paginiChemical Engineering Projects List For Final YearRajnikant Tiwari67% (6)
- Effectiveness and Safety of Dabigatran, Rivaroxaban, and Apixaban Versus Warfarin in Nonvalvular Atrial FibrillationDocument18 paginiEffectiveness and Safety of Dabigatran, Rivaroxaban, and Apixaban Versus Warfarin in Nonvalvular Atrial FibrillationgaryÎncă nu există evaluări
- Graham The American Journal of MedicineDocument21 paginiGraham The American Journal of MedicinemadrugagalanfÎncă nu există evaluări
- Comparison of Dabigatran Versus Warfarin TreatmentDocument7 paginiComparison of Dabigatran Versus Warfarin TreatmentDivyesh AmarsedaÎncă nu există evaluări
- Ecr 12 1 40Document6 paginiEcr 12 1 40Ahmed MohammedÎncă nu există evaluări
- Effectiveness and Safety of Dabigatran, Rivaroxaban, and Apixaban Versus Warfarin in Nonvalvular Atrial FibrillationDocument18 paginiEffectiveness and Safety of Dabigatran, Rivaroxaban, and Apixaban Versus Warfarin in Nonvalvular Atrial FibrillationJUAN SEBASTIAN CLAVIJO CASTELLANOSÎncă nu există evaluări
- Jeong DKK, 2019Document8 paginiJeong DKK, 2019sri noviyanty yusufÎncă nu există evaluări
- Apixaban For Patients With Atrial Fibrillation On Hemodialysis: A Multicenter Randomized Controlled TrialDocument11 paginiApixaban For Patients With Atrial Fibrillation On Hemodialysis: A Multicenter Randomized Controlled TrialMedicina UPBÎncă nu există evaluări
- Ischemic Stroke and Intracranial Hemorrhage With Aspirin, Dabigatran, and WarfarinDocument9 paginiIschemic Stroke and Intracranial Hemorrhage With Aspirin, Dabigatran, and WarfarinNur Syamsiah MÎncă nu există evaluări
- Editorial Caravaggio Apixaban en Cáncer y ETVDocument3 paginiEditorial Caravaggio Apixaban en Cáncer y ETVSANTIAGO FOREROÎncă nu există evaluări
- 345 FullDocument8 pagini345 FullwisgeorgekwokÎncă nu există evaluări
- PIONEERstudy 2016Document12 paginiPIONEERstudy 2016Jose Enrique Valecillos MorenoÎncă nu există evaluări
- Rivaroxaban Vs Warfarin Sodium in The Ultra-Early Period After Atrial Fibrillation-Related Mild Ischemic StrokeDocument10 paginiRivaroxaban Vs Warfarin Sodium in The Ultra-Early Period After Atrial Fibrillation-Related Mild Ischemic StrokeRoberto López MataÎncă nu există evaluări
- Review of Clinical Studies On Angiotensin II Receptor Blockers and Risk of CancerDocument6 paginiReview of Clinical Studies On Angiotensin II Receptor Blockers and Risk of CancerRisa MuthmainahÎncă nu există evaluări
- 28720644: Effects of Non-Vitamin K Antagonist Oral Anticoagulants Versus Warfarin in Patients With Atrial Fibrillation and Valvular Heart Disease A Systematic Review and Meta-AnalysisDocument12 pagini28720644: Effects of Non-Vitamin K Antagonist Oral Anticoagulants Versus Warfarin in Patients With Atrial Fibrillation and Valvular Heart Disease A Systematic Review and Meta-AnalysisaleksÎncă nu există evaluări
- Selective Serotonin Reuptake Inhibitors and Bleeding Risk in Anticoagulated Patients With Atrial FibrillationDocument9 paginiSelective Serotonin Reuptake Inhibitors and Bleeding Risk in Anticoagulated Patients With Atrial FibrillationGiancarlos GuzmanÎncă nu există evaluări
- Rivaroxaban Versus Apixaban For Stroke Prevention in Atrial FibrillationDocument10 paginiRivaroxaban Versus Apixaban For Stroke Prevention in Atrial FibrillationRicardo BarcoÎncă nu există evaluări
- Rivaroxavan en Fa ValvularDocument5 paginiRivaroxavan en Fa Valvularcarlos pardoÎncă nu există evaluări
- Anticoagulantes Orales e Infarto Agudo Miocardio 2018 Carta EditorialDocument2 paginiAnticoagulantes Orales e Infarto Agudo Miocardio 2018 Carta EditorialRenzo RosalesÎncă nu există evaluări
- Rivaroxaban Versus Dabigatran or Warfarin in Real-World Studies of Stroke Prevention in Atrial FibrillationDocument21 paginiRivaroxaban Versus Dabigatran or Warfarin in Real-World Studies of Stroke Prevention in Atrial FibrillationMerDeKÎncă nu există evaluări
- Re LyDocument13 paginiRe LyDilawar JanÎncă nu există evaluări
- 361 2012 LaHayeDocument9 pagini361 2012 LaHayeOscar PonceÎncă nu există evaluări
- Aer 04 100Document8 paginiAer 04 100I Al WÎncă nu există evaluări
- 2020 Asociación Entre El Uso de Warfarina para La Fibrilación Auricular y Los Resultados Entre Pacientes Con Enfermedad Renal en Etapa TerminalDocument13 pagini2020 Asociación Entre El Uso de Warfarina para La Fibrilación Auricular y Los Resultados Entre Pacientes Con Enfermedad Renal en Etapa TerminalbernardoÎncă nu există evaluări
- Assessing The Risk of Bleeding in Patients With Atrial FibrillationDocument8 paginiAssessing The Risk of Bleeding in Patients With Atrial FibrillationAngga Aryo LukmantoÎncă nu există evaluări
- Enoxaparin Versus Unfractionated Heparin in Elective Percutaneous Coronary InterventionDocument12 paginiEnoxaparin Versus Unfractionated Heparin in Elective Percutaneous Coronary InterventionMuhammad FarisÎncă nu există evaluări
- Effect of Rivaroxaban Vs Enoxaparin On Major Cardiac Adverse Events and Bleeding Risk in The Acute Phase of Acute Coronary Syndrome PDFDocument13 paginiEffect of Rivaroxaban Vs Enoxaparin On Major Cardiac Adverse Events and Bleeding Risk in The Acute Phase of Acute Coronary Syndrome PDFKardiologi ManadoÎncă nu există evaluări
- Riva Rox AbanDocument11 paginiRiva Rox AbanMr. LÎncă nu există evaluări
- Doacs in Patients With Mitral Stenosis and Atrial FibrillationDocument3 paginiDoacs in Patients With Mitral Stenosis and Atrial FibrillationNasriÎncă nu există evaluări
- Rivaroxaban in Rheumatic Heart Disease - Associated Atrial FibrillationDocument11 paginiRivaroxaban in Rheumatic Heart Disease - Associated Atrial FibrillationEstevão CaminhaÎncă nu există evaluări
- Antagonist Oral AnticoagulantsDocument66 paginiAntagonist Oral Anticoagulantsbagheera316Încă nu există evaluări
- NEJM 2017 Comentario Braunwald2017Document2 paginiNEJM 2017 Comentario Braunwald2017Francisca Javiera Yáñez VidalÎncă nu există evaluări
- Commander HFDocument11 paginiCommander HFhairos.izhaÎncă nu există evaluări
- JAH3 11 E025723Document36 paginiJAH3 11 E025723ResidenPatKlin Juli2022Încă nu există evaluări
- Fsurg 10 1285553Document11 paginiFsurg 10 1285553William ChokÎncă nu există evaluări
- J Ahj 2006 06 024Document7 paginiJ Ahj 2006 06 024Alexandra RosaÎncă nu există evaluări
- Afire Articulo OriginalDocument11 paginiAfire Articulo OriginalElvira AnitaÎncă nu există evaluări
- Rivaroxaban in Patients With Atrial Fibrillation and A Bioprosthetic Mitral ValveDocument11 paginiRivaroxaban in Patients With Atrial Fibrillation and A Bioprosthetic Mitral ValveJuan JoseÎncă nu există evaluări
- Comparisons Between Oral Anticoagulants Among Older Nonvalvular Atrial Fibrillation PatientsDocument10 paginiComparisons Between Oral Anticoagulants Among Older Nonvalvular Atrial Fibrillation PatientsmadrugagalanfÎncă nu există evaluări
- Matanalisis ACODocument8 paginiMatanalisis ACOMarcelo AbrahamÎncă nu există evaluări
- TCP15 11MarcyTruongRaiDocument14 paginiTCP15 11MarcyTruongRaiadri20121989Încă nu există evaluări
- 10 1001@jamacardio 2020 4390Document9 pagini10 1001@jamacardio 2020 4390William ChokÎncă nu există evaluări
- Matsumoto2014 PDFDocument6 paginiMatsumoto2014 PDFNur Syamsiah MÎncă nu există evaluări
- Antithrombotic Therapy After Revascularization in Patients With Peripheral Arterial Disease: What Is Here, What Is NextDocument12 paginiAntithrombotic Therapy After Revascularization in Patients With Peripheral Arterial Disease: What Is Here, What Is NextenviÎncă nu există evaluări
- COMPASS by RISK STRATDocument10 paginiCOMPASS by RISK STRATMiguel GonzalezÎncă nu există evaluări
- Effectiveness and Safety of Direct Oral Anticoagulants in The Secondary Stroke Prevention of Elderly PatientsDocument9 paginiEffectiveness and Safety of Direct Oral Anticoagulants in The Secondary Stroke Prevention of Elderly PatientsLiam HudnikÎncă nu există evaluări
- Strokeaha 120 032704Document11 paginiStrokeaha 120 032704Norlando RuizÎncă nu există evaluări
- Circulation 2015 Avezum 624 32Document10 paginiCirculation 2015 Avezum 624 32Ernesto Ventura QuirogaÎncă nu există evaluări
- AC After StrokeDocument6 paginiAC After StrokeDileepa chathurangaÎncă nu există evaluări
- Unanswered Questions During The Live EventDocument9 paginiUnanswered Questions During The Live Eventyash_acharya007Încă nu există evaluări
- Health Services and Outcomes ResearchDocument10 paginiHealth Services and Outcomes ResearchRJMÎncă nu există evaluări
- The Reply AjmDocument2 paginiThe Reply AjmRaynolds Geraldy's photoÎncă nu există evaluări
- Jama Sidhu 2022 Oi 220087 1668452383.53768Document9 paginiJama Sidhu 2022 Oi 220087 1668452383.53768Karina AngelÎncă nu există evaluări
- Stroke Prevention in Atrial Fibrillation A Systematic ReviewDocument13 paginiStroke Prevention in Atrial Fibrillation A Systematic ReviewSebastian PierreÎncă nu există evaluări
- Debus Et Al 2021 Effect of Rivaroxaban and Aspirin in Patients With Peripheral Artery Disease Undergoing SurgicalDocument13 paginiDebus Et Al 2021 Effect of Rivaroxaban and Aspirin in Patients With Peripheral Artery Disease Undergoing SurgicalWilliam ChokÎncă nu există evaluări
- Apixaban With Antiplatelet Therapy After Acute Coronary SyndromeDocument10 paginiApixaban With Antiplatelet Therapy After Acute Coronary SyndromeAndi Soraya PurnamandaÎncă nu există evaluări
- Rivaroxaban ArticleDocument12 paginiRivaroxaban ArticleA. RaufÎncă nu există evaluări
- Anticoagulant in Atrial Fibrillation Patients With Prior IntracranialDocument7 paginiAnticoagulant in Atrial Fibrillation Patients With Prior IntracranialWilliam BarreraÎncă nu există evaluări
- 235 FullDocument8 pagini235 Fullsri noviyanty yusufÎncă nu există evaluări
- Complementary and Alternative Medical Lab Testing Part 3: CardiologyDe la EverandComplementary and Alternative Medical Lab Testing Part 3: CardiologyEvaluare: 1 din 5 stele1/5 (1)
- Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Synopsis of The 2017 American College of Cardiology:American Heart Association Hypertension GuidelineDocument10 paginiPrevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Synopsis of The 2017 American College of Cardiology:American Heart Association Hypertension GuidelineRoberto López MataÎncă nu există evaluări
- Best Clinical Practice: AnaphylaxisDocument6 paginiBest Clinical Practice: AnaphylaxisputriÎncă nu există evaluări
- 2017 ACC Expert Consensus Decision Pathway For Optimization of Heart Failure TreatmentDocument30 pagini2017 ACC Expert Consensus Decision Pathway For Optimization of Heart Failure TreatmentRoberto López MataÎncă nu există evaluări
- Hyperglycemic CrisisDocument9 paginiHyperglycemic CrisisRoberto López MataÎncă nu există evaluări
- HTN Emergencies and UrgenciesDocument14 paginiHTN Emergencies and UrgenciesRoberto López MataÎncă nu există evaluări
- Necrotizing Soft-Tissue InfectionsDocument13 paginiNecrotizing Soft-Tissue InfectionsRoberto López MataÎncă nu există evaluări
- Top 10 Myths Regarding The Diagnosis and Treatment of CellulitisDocument8 paginiTop 10 Myths Regarding The Diagnosis and Treatment of CellulitisRoberto López MataÎncă nu există evaluări
- ADA 2018 Diabetes CareDocument150 paginiADA 2018 Diabetes CareRoberto López Mata100% (1)
- Fluid Therapy Options and Rational SelectionDocument13 paginiFluid Therapy Options and Rational SelectionRoberto López MataÎncă nu există evaluări
- Update On The Management of Venous ThromboembolismDocument8 paginiUpdate On The Management of Venous ThromboembolismRoberto López MataÎncă nu există evaluări
- Diagnosis and Treatment of HyperkalemiaDocument9 paginiDiagnosis and Treatment of HyperkalemiaRoberto López MataÎncă nu există evaluări
- Uric Acid Is A Strong Risk Marker For Developing Hypertension From PrehypertensionDocument16 paginiUric Acid Is A Strong Risk Marker For Developing Hypertension From PrehypertensionRoberto López MataÎncă nu există evaluări
- The Use of Cephalosporins in Penicillin-Allergic Patients - A Literature ReviewDocument9 paginiThe Use of Cephalosporins in Penicillin-Allergic Patients - A Literature ReviewRoberto López MataÎncă nu există evaluări
- Pathophysiology of Septic ShockDocument19 paginiPathophysiology of Septic ShockRoberto López MataÎncă nu există evaluări
- The Dark Sides of Fuid Administration in The Critically Ill PatientDocument3 paginiThe Dark Sides of Fuid Administration in The Critically Ill PatientRoberto López MataÎncă nu există evaluări
- A Test in Context - D-DimerDocument10 paginiA Test in Context - D-DimerRoberto López MataÎncă nu există evaluări
- Sudden Cardiac Arrest During Participation in Competitive SportsDocument11 paginiSudden Cardiac Arrest During Participation in Competitive SportsRoberto López MataÎncă nu există evaluări
- Hepatitis B Vaccination, Screening, and Linkage To Care - Best Practice Advice From The American College of Physicians and The Centers For Disease Control and PreventionDocument12 paginiHepatitis B Vaccination, Screening, and Linkage To Care - Best Practice Advice From The American College of Physicians and The Centers For Disease Control and PreventionRoberto López MataÎncă nu există evaluări
- Atrial Fibrillation and HypertensionDocument17 paginiAtrial Fibrillation and HypertensionRoberto López MataÎncă nu există evaluări
- Diuretic Treatment in Heart FailureDocument12 paginiDiuretic Treatment in Heart FailureRoberto López Mata100% (1)
- The Role of Nitroglycerin and Other Nitrogen Oxides in Cardiovascular TherapeuticsDocument18 paginiThe Role of Nitroglycerin and Other Nitrogen Oxides in Cardiovascular TherapeuticsRoberto López MataÎncă nu există evaluări
- Rivaroxaban Vs Warfarin Sodium in The Ultra-Early Period After Atrial Fibrillation-Related Mild Ischemic StrokeDocument10 paginiRivaroxaban Vs Warfarin Sodium in The Ultra-Early Period After Atrial Fibrillation-Related Mild Ischemic StrokeRoberto López MataÎncă nu există evaluări
- Effects of Acarbose On Cardiovascular and Diabetes Outcomes in Patients With Coronary Heart Disease and Impaired Glucose Tolerance (ACE) - A Randomised, Double-Blind, Placebo-Controlled TrialDocument10 paginiEffects of Acarbose On Cardiovascular and Diabetes Outcomes in Patients With Coronary Heart Disease and Impaired Glucose Tolerance (ACE) - A Randomised, Double-Blind, Placebo-Controlled TrialRoberto López MataÎncă nu există evaluări
- Acute Monocular Vision LossDocument9 paginiAcute Monocular Vision LossRoberto López MataÎncă nu există evaluări
- 2015 ESC Guidelines For The Diagnosis and Management of Pericardial DiseasesDocument44 pagini2015 ESC Guidelines For The Diagnosis and Management of Pericardial DiseasesRoberto López MataÎncă nu există evaluări
- Synopsis of The 2017 U.S. Department of Veterans Affairs: Management of Type 2 Diabetes MellitusDocument10 paginiSynopsis of The 2017 U.S. Department of Veterans Affairs: Management of Type 2 Diabetes MellitusRoberto López MataÎncă nu există evaluări
- Effects on the Incidence of Cardiovascular Events of the Addition of Pioglitazone Versus Sulfonylureas in Patients With Type 2 Diabetes Inadequately Controlled With Metformin (TOSCA.it)- A Randomised, Multicentre TrialDocument11 paginiEffects on the Incidence of Cardiovascular Events of the Addition of Pioglitazone Versus Sulfonylureas in Patients With Type 2 Diabetes Inadequately Controlled With Metformin (TOSCA.it)- A Randomised, Multicentre TrialRoberto López MataÎncă nu există evaluări
- Evaluation and Management of Lower-Extremity UlcersDocument9 paginiEvaluation and Management of Lower-Extremity UlcersRoberto López MataÎncă nu există evaluări
- Dual Antithrombotic Therapy With Dabigatran After PCI in Atrial FibrillationDocument12 paginiDual Antithrombotic Therapy With Dabigatran After PCI in Atrial FibrillationRoberto López MataÎncă nu există evaluări
- 2020 ROTH IRA 229664667 Form 5498Document2 pagini2020 ROTH IRA 229664667 Form 5498hk100% (1)
- Lab Manual PDFDocument68 paginiLab Manual PDFSantino AwetÎncă nu există evaluări
- Organogram - Qa / QC: Srinivasan SrinivasanDocument4 paginiOrganogram - Qa / QC: Srinivasan SrinivasanGowtham VenkatÎncă nu există evaluări
- 10 2005 Dec QDocument6 pagini10 2005 Dec Qspinster40% (1)
- Lesson 1 - Intro To Highway EngineeringDocument15 paginiLesson 1 - Intro To Highway EngineeringSaoirseÎncă nu există evaluări
- HUM110 Gilgamesh EssayDocument4 paginiHUM110 Gilgamesh EssaynsmeganÎncă nu există evaluări
- Fill The Gaps With The Correct WordsDocument2 paginiFill The Gaps With The Correct WordsAlayza ChangÎncă nu există evaluări
- Standards Spec Brochure ME WEBDocument44 paginiStandards Spec Brochure ME WEBReza TambaÎncă nu există evaluări
- Method StatementDocument29 paginiMethod StatementZakwan Hisyam100% (1)
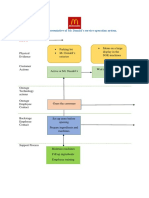
- Blueprint Huynh My Ky Duyen 2022 McDonald'sDocument2 paginiBlueprint Huynh My Ky Duyen 2022 McDonald'sHuỳnh Mỹ Kỳ DuyênÎncă nu există evaluări
- Marine Trans Owners Manual 1016313 RevH 0116 CDDocument200 paginiMarine Trans Owners Manual 1016313 RevH 0116 CDMarco Aurelio BarbosaÎncă nu există evaluări
- Fast FashionDocument9 paginiFast FashionTeresa GonzalezÎncă nu există evaluări
- Penilaian Akhir TahunDocument4 paginiPenilaian Akhir TahunRestu Suci UtamiÎncă nu există evaluări
- Ras Shastra PPT 6Document10 paginiRas Shastra PPT 6Soham BhureÎncă nu există evaluări
- Parche CRP 65 - Ficha Técnica - en InglesDocument2 paginiParche CRP 65 - Ficha Técnica - en IngleserwinvillarÎncă nu există evaluări
- Psychoanalysis AND History: Freud: Dreaming, Creativity and TherapyDocument2 paginiPsychoanalysis AND History: Freud: Dreaming, Creativity and TherapyJuan David Millán MendozaÎncă nu există evaluări
- Tamilnadu Shop and Establishment ActDocument6 paginiTamilnadu Shop and Establishment ActShiny VargheesÎncă nu există evaluări
- NG Teng Fong Discharge DocumentsDocument14 paginiNG Teng Fong Discharge DocumentsAnonymous yGwMIPJRawÎncă nu există evaluări
- Sop For Enlistment of Engineering ConsultantsDocument1 paginăSop For Enlistment of Engineering Consultantssatheb319429Încă nu există evaluări
- Yogananda Scientific HealingDocument47 paginiYogananda Scientific HealingSagar Pandya100% (4)
- Heteropolyacids FurfuralacetoneDocument12 paginiHeteropolyacids FurfuralacetonecligcodiÎncă nu există evaluări
- Itrogen: by Deborah A. KramerDocument18 paginiItrogen: by Deborah A. KramernycÎncă nu există evaluări
- Transfer and Business Taxation SyllabusDocument5 paginiTransfer and Business Taxation SyllabusamqqndeahdgeÎncă nu există evaluări
- Rules For State Competitions and Iabf Approved TournamentsDocument56 paginiRules For State Competitions and Iabf Approved TournamentsQuality management systems documentsÎncă nu există evaluări
- Sav4747 PDFDocument49 paginiSav4747 PDFAndres Antonio Moreno CastroÎncă nu există evaluări
- Iomm VFD-3 030112Document100 paginiIomm VFD-3 030112Alexander100% (1)
- Dr. Nastiti K - Manajemen Asma Pada Anak 2018 PDFDocument72 paginiDr. Nastiti K - Manajemen Asma Pada Anak 2018 PDFagnesspratiwiÎncă nu există evaluări
- Current Concepts of Enzyme Histochemistry in Modern PathologyDocument11 paginiCurrent Concepts of Enzyme Histochemistry in Modern PathologyRosa AquinoÎncă nu există evaluări