S-ar putea să vă placă și
- Psychiatry PhyseoDocument60 paginiPsychiatry PhyseoGautam ManoharÎncă nu există evaluări
- HerbsDocument476 paginiHerbsVishnu Ronaldus Narayan100% (1)
- Data Interpretation For Medical Students PDFDocument905 paginiData Interpretation For Medical Students PDFMarÎncă nu există evaluări
- Histopathology of Preclinical Toxicity Studies: Interpretation and Relevance in Drug Safety EvaluationDe la EverandHistopathology of Preclinical Toxicity Studies: Interpretation and Relevance in Drug Safety EvaluationÎncă nu există evaluări
- Surveillance PDFDocument48 paginiSurveillance PDFadhar100% (1)
- Fast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeDe la EverandFast Facts: Complex Perianal Fistulas in Crohn's Disease: A multidisciplinary approach to a clinical challengeÎncă nu există evaluări
- HELLP SyndromeDocument3 paginiHELLP SyndromeWidyawati TjahjadiÎncă nu există evaluări
- Herbal MedicineDocument8 paginiHerbal MedicineStephanie Joy EscalaÎncă nu există evaluări
- Top Trials in Gastroenterology & HepatologyDe la EverandTop Trials in Gastroenterology & HepatologyEvaluare: 4.5 din 5 stele4.5/5 (7)
- NGT Feeding ChecklistDocument4 paginiNGT Feeding ChecklistCee Sanchez100% (6)
- Outcome and Clinical Characteristics in Pleural Empyema: A Retrospective StudyDocument7 paginiOutcome and Clinical Characteristics in Pleural Empyema: A Retrospective StudylestarisurabayaÎncă nu există evaluări
- Gfac 227Document8 paginiGfac 227Cristina Adriana PopaÎncă nu există evaluări
- Septic ShockDocument12 paginiSeptic ShockPatrick CommettantÎncă nu există evaluări
- Nejm Trial 2023Document11 paginiNejm Trial 2023Sachin KumarÎncă nu există evaluări
- Pneumonia 5Document6 paginiPneumonia 5furqan92Încă nu există evaluări
- Nerjm SesionDocument12 paginiNerjm SesionjorgeÎncă nu există evaluări
- Response To Methylprednisolone Bolus in Children Treated For Nephrotic Syndrome at The Pediatric Nephrology Unit in AbidjanDocument5 paginiResponse To Methylprednisolone Bolus in Children Treated For Nephrotic Syndrome at The Pediatric Nephrology Unit in AbidjanIJAR JOURNALÎncă nu există evaluări
- Tugas RCT SenaDocument10 paginiTugas RCT SenaArfad El HabibieÎncă nu există evaluări
- Fatores Risco PEG 2018Document10 paginiFatores Risco PEG 2018Kiki PuchiÎncă nu există evaluări
- Pneumonia 4Document10 paginiPneumonia 4furqan92Încă nu există evaluări
- 2023 - Hydrocortisone in Severe CommunityDocument11 pagini2023 - Hydrocortisone in Severe CommunitygiseladlrÎncă nu există evaluări
- Clinical Outcomes of Esophagogastroduodenoscopy In.27Document6 paginiClinical Outcomes of Esophagogastroduodenoscopy In.27Agung KaryawinaraÎncă nu există evaluări
- Jurnal 4Document7 paginiJurnal 4Lutfi MalefoÎncă nu există evaluări
- Restrictive Fluids in Septic Shock. NEJM 2022Document12 paginiRestrictive Fluids in Septic Shock. NEJM 2022neeraj SinghÎncă nu există evaluări
- Corticosteroids in The Treatment of Vestibular Neuritis: A Systematic Review and Meta-AnalysisDocument7 paginiCorticosteroids in The Treatment of Vestibular Neuritis: A Systematic Review and Meta-AnalysisshiloinÎncă nu există evaluări
- Acute Pyelonephritis in Adults: A Case Series of 223 PatientsDocument6 paginiAcute Pyelonephritis in Adults: A Case Series of 223 PatientsshiaÎncă nu există evaluări
- Management of Necrotizing Otitis Externa: Our Experience With Forty-Three PatientsDocument5 paginiManagement of Necrotizing Otitis Externa: Our Experience With Forty-Three Patientsmenik ayuÎncă nu există evaluări
- GNL 10 581Document6 paginiGNL 10 581Teh NuraqilahÎncă nu există evaluări
- Journal Read ChiaDocument14 paginiJournal Read ChiaChris Tine ChiaÎncă nu există evaluări
- Risk Factors For Necrotizing Enterocolitis Associated MortalityDocument7 paginiRisk Factors For Necrotizing Enterocolitis Associated MortalityvaleriaÎncă nu există evaluări
- Ramirez 2013Document10 paginiRamirez 2013Nadia Farah FadhilaÎncă nu există evaluări
- Silent NightDocument6 paginiSilent NightApril Rae Obregon GarcesÎncă nu există evaluări
- Original Article: Key WordsDocument9 paginiOriginal Article: Key WordsykommÎncă nu există evaluări
- CC 12918Document59 paginiCC 12918Romica MarcanÎncă nu există evaluări
- Azitromicyn COPDDocument10 paginiAzitromicyn COPDLucrécia BórgiaÎncă nu există evaluări
- AygunDocument5 paginiAygunotheasÎncă nu există evaluări
- Plasma Conv Full ArticleDocument9 paginiPlasma Conv Full ArticlemahamedicÎncă nu există evaluări
- Changes in Acute Poststreptococcal Glomerulonephritis: An Observation Study at A Single Korean Hospital Over Two DecadesDocument6 paginiChanges in Acute Poststreptococcal Glomerulonephritis: An Observation Study at A Single Korean Hospital Over Two DecadesTimothy Eduard A. SupitÎncă nu există evaluări
- Meningitis TBDocument11 paginiMeningitis TBErni Yessyca SimamoraÎncă nu există evaluări
- Detection of Recurrent Oral Squamous Cell Carcinoma by (F) - 2-Fluorodeoxyglucose-Positron Emission TomographyDocument9 paginiDetection of Recurrent Oral Squamous Cell Carcinoma by (F) - 2-Fluorodeoxyglucose-Positron Emission TomographyMindaugas TÎncă nu există evaluări
- Srinivasan 2004Document8 paginiSrinivasan 2004Dr XÎncă nu există evaluări
- Ferrer 2008Document10 paginiFerrer 2008yusÎncă nu există evaluări
- Complications of Pancreatic SurgeryDocument5 paginiComplications of Pancreatic Surgeryhenok seifeÎncă nu există evaluări
- Chlo Ramp He NicolDocument6 paginiChlo Ramp He NicolDivika ShilvanaÎncă nu există evaluări
- A Randomized Clinical TrialDocument11 paginiA Randomized Clinical TrialRandy PrayogoÎncă nu există evaluări
- Iihyuyu6756e54tw5w3553w5et6yfug5757 Jgut75Document6 paginiIihyuyu6756e54tw5w3553w5et6yfug5757 Jgut75RIBÎncă nu există evaluări
- 2009hetrase CCMDocument12 pagini2009hetrase CCMgiseladelarosa2006Încă nu există evaluări
- Aborto septico Lanari-USA ICM 2004Document6 paginiAborto septico Lanari-USA ICM 2004pastorizaariana25Încă nu există evaluări
- Inhibidor Bomba de Protones e Infecci - NDocument10 paginiInhibidor Bomba de Protones e Infecci - NSMIBA Medicina100% (1)
- Azithromycin For Prevention of Exacerbations of COPDDocument10 paginiAzithromycin For Prevention of Exacerbations of COPDAJÎncă nu există evaluări
- Traumatic Posterior Fossa Epidural Hematomas in Children: Experience With 48 Cases and A Review of The LiteratureDocument7 paginiTraumatic Posterior Fossa Epidural Hematomas in Children: Experience With 48 Cases and A Review of The LiteratureSusy NolesÎncă nu există evaluări
- Bleeding peptic ulcer epidemiology and prognosisDocument8 paginiBleeding peptic ulcer epidemiology and prognosisJain KasparÎncă nu există evaluări
- Traa 144Document9 paginiTraa 144RashifÎncă nu există evaluări
- Use of Ketorolac Is Associated With Decreased Pneumonia Following Rib FracturesDocument7 paginiUse of Ketorolac Is Associated With Decreased Pneumonia Following Rib Fracturesracut_khansatraÎncă nu există evaluări
- Impact of Postoperative Morbidity On Long-Term Survival After OesophagectomyDocument10 paginiImpact of Postoperative Morbidity On Long-Term Survival After OesophagectomyPutri PadmosuwarnoÎncă nu există evaluări
- Palliative and End-Of-Life Care For Children With DiffuseDocument7 paginiPalliative and End-Of-Life Care For Children With DiffuseLetticia BenthinÎncă nu există evaluări
- Estensis Sub 9Document5 paginiEstensis Sub 9Nicolás HenaoÎncă nu există evaluări
- s13054 019 2354 4Document11 paginis13054 019 2354 4Residentes PediatríaÎncă nu există evaluări
- Jurnal FixDocument2 paginiJurnal Fixuflah_Încă nu există evaluări
- Efektivitas Pemberian CGF 40% Dalam Mempercepat Peningkatan Trombosit Pada Penderita Demam Berdarah DengueDocument9 paginiEfektivitas Pemberian CGF 40% Dalam Mempercepat Peningkatan Trombosit Pada Penderita Demam Berdarah DengueHenny BarutuÎncă nu există evaluări
- Ye 2014Document8 paginiYe 2014dickypranataÎncă nu există evaluări
- Interstitial Lung Disease After Pleurodesis For Malignant Pleural EffusionDocument7 paginiInterstitial Lung Disease After Pleurodesis For Malignant Pleural EffusionMomoraÎncă nu există evaluări
- Chronic Kidney Disease Is Associated With A Higher 90-Day Mortality Than Other Chronic Medical Conditions in Patients With SepsisDocument8 paginiChronic Kidney Disease Is Associated With A Higher 90-Day Mortality Than Other Chronic Medical Conditions in Patients With Sepsisida ayu agung WijayantiÎncă nu există evaluări
- A Simple Prognostic Score For Risk Assessment in Patients With Acute PancreatitisDocument6 paginiA Simple Prognostic Score For Risk Assessment in Patients With Acute PancreatitisGeorgiana CrisuÎncă nu există evaluări
- Hodgkin Lymphoma: A Comprehensive OverviewDe la EverandHodgkin Lymphoma: A Comprehensive OverviewAndreas EngertÎncă nu există evaluări
- Endoscopy in Pediatric Inflammatory Bowel DiseaseDe la EverandEndoscopy in Pediatric Inflammatory Bowel DiseaseLuigi Dall'OglioÎncă nu există evaluări
- Controlled Zn2+-Triggered Drug Release by Preferred Coordination of Open Active Sites Within Functionalization Indium Metal Organic FrameworksDocument27 paginiControlled Zn2+-Triggered Drug Release by Preferred Coordination of Open Active Sites Within Functionalization Indium Metal Organic FrameworksFebyan AbotÎncă nu există evaluări
- NPP 2013297 ADocument8 paginiNPP 2013297 AFebyan AbotÎncă nu există evaluări
- Inflammation: The Common Pathway of Stress-Related Diseases: Yun-Zi Liu Yun-Xia Wang Chun-Lei JiangDocument11 paginiInflammation: The Common Pathway of Stress-Related Diseases: Yun-Zi Liu Yun-Xia Wang Chun-Lei JiangFebyan AbotÎncă nu există evaluări
- Combination of PPI With A Prokinetic Drug in Gastroesophageal Reflux DiseaseDocument19 paginiCombination of PPI With A Prokinetic Drug in Gastroesophageal Reflux DiseaseFebyan AbotÎncă nu există evaluări
- Controlled Zn2+-Triggered Drug Release by Preferred Coordination of Open Active Sites Within Functionalization Indium Metal Organic FrameworksDocument27 paginiControlled Zn2+-Triggered Drug Release by Preferred Coordination of Open Active Sites Within Functionalization Indium Metal Organic FrameworksFebyan AbotÎncă nu există evaluări
- Mud I Gonda 2013Document3 paginiMud I Gonda 2013Febyan AbotÎncă nu există evaluări
- 278 Management of Paediatric Sepsis PDFDocument10 pagini278 Management of Paediatric Sepsis PDFAfrizal AdzÎncă nu există evaluări
- Salicil Acid DermaDocument9 paginiSalicil Acid DermaFebyan AbotÎncă nu există evaluări
- VitiligoDocument13 paginiVitiligoFebyan AbotÎncă nu există evaluări
- Editorial: Stress Induced Neuroplasticity and Mental DisordersDocument4 paginiEditorial: Stress Induced Neuroplasticity and Mental DisordersFebyan AbotÎncă nu există evaluări
- 10 1016@j Psyneuen 2017 09 007Document43 pagini10 1016@j Psyneuen 2017 09 007Febyan AbotÎncă nu există evaluări
- Filip Ventorp Inflammatory Mechanisms of Depression and Suicidal BehaviorDocument113 paginiFilip Ventorp Inflammatory Mechanisms of Depression and Suicidal BehaviorFebyan AbotÎncă nu există evaluări
- 25122012012424Document6 pagini25122012012424Febyan AbotÎncă nu există evaluări
- Tulisan Nyeri Saraf Adelyna MelialaDocument5 paginiTulisan Nyeri Saraf Adelyna MelialaFebyan AbotÎncă nu există evaluări
- Icmje Recommendations PDFDocument17 paginiIcmje Recommendations PDFFebyan AbotÎncă nu există evaluări
- 0004 282X Anp 73 5 0415Document5 pagini0004 282X Anp 73 5 0415Febyan AbotÎncă nu există evaluări
- Patof UTAMADocument12 paginiPatof UTAMAFebyan AbotÎncă nu există evaluări
- Aime201703210 M161785Document10 paginiAime201703210 M161785Febyan AbotÎncă nu există evaluări
- 78Document5 pagini78Febyan AbotÎncă nu există evaluări
- 78Document5 pagini78Febyan AbotÎncă nu există evaluări
- Hap Vap Guidelines 2016 PDFDocument51 paginiHap Vap Guidelines 2016 PDFJerryEddyaPutraBoerÎncă nu există evaluări
- The Effect of Green Tea Extract Supplementation On Liver Enzymes in Patients With Nonalcoholic Fatty Liver DiseaseDocument6 paginiThe Effect of Green Tea Extract Supplementation On Liver Enzymes in Patients With Nonalcoholic Fatty Liver DiseaseFebyan AbotÎncă nu există evaluări
- Review Article: Signal Transductions and Nonalcoholic Fatty Liver: A Mini-ReviewDocument8 paginiReview Article: Signal Transductions and Nonalcoholic Fatty Liver: A Mini-ReviewFebyan AbotÎncă nu există evaluări
- 975 FullDocument8 pagini975 FullFebyan AbotÎncă nu există evaluări
- 1 s2.0 S1201971211000944 MainDocument6 pagini1 s2.0 S1201971211000944 MainFebyan AbotÎncă nu există evaluări
- Piis0016510714001515Document8 paginiPiis0016510714001515Febyan AbotÎncă nu există evaluări
- Endoscopy in The ElderlyDocument7 paginiEndoscopy in The ElderlyFebyan AbotÎncă nu există evaluări
- Journal of Molecular SignalingDocument11 paginiJournal of Molecular SignalingFebyan AbotÎncă nu există evaluări
- Green Tea Polyphenol Epigallocatechin-3-Gallate Ameliorates Insulin Resistance in Non-Alcoholic Fatty Liver Disease MiceDocument9 paginiGreen Tea Polyphenol Epigallocatechin-3-Gallate Ameliorates Insulin Resistance in Non-Alcoholic Fatty Liver Disease MiceFebyan AbotÎncă nu există evaluări
- Medicinal Use of Ajwain or Carom SeedsDocument5 paginiMedicinal Use of Ajwain or Carom SeedsSanjay PatilÎncă nu există evaluări
- The Thorax and Lungs - BATESDocument4 paginiThe Thorax and Lungs - BATESsitalcoolk100% (2)
- Reforms Corresponding To The Population Ageing: The Case of JapanDocument22 paginiReforms Corresponding To The Population Ageing: The Case of JapanADBI EventsÎncă nu există evaluări
- Clinic Note Summary for Mr. Carl EwingDocument2 paginiClinic Note Summary for Mr. Carl EwingCara Joy SeguinÎncă nu există evaluări
- Eritro Papulo Skuamosa 2021Document47 paginiEritro Papulo Skuamosa 2021Yolanda Agnesia Purba0% (1)
- Ceftriaxone: Antibiotic ClassDocument2 paginiCeftriaxone: Antibiotic ClassTanjung PrabandariÎncă nu există evaluări
- Impact of Advertising Food To Pakistan Television On ChildrenDocument14 paginiImpact of Advertising Food To Pakistan Television On Childrenalim110Încă nu există evaluări
- Formulation of Pulpal and Periradicular DiagnosesDocument3 paginiFormulation of Pulpal and Periradicular DiagnosesJoyce LimÎncă nu există evaluări
- Physiologic and Psychologic Stressors Nurses Must RecognizeDocument5 paginiPhysiologic and Psychologic Stressors Nurses Must RecognizeMilcah NuylesÎncă nu există evaluări
- Microbiology Mock Board RationalizationDocument228 paginiMicrobiology Mock Board RationalizationCla NuvalÎncă nu există evaluări
- Colon Cleansing, Cleanse - Net Colon Plaque - Mucoid PlaqueDocument15 paginiColon Cleansing, Cleanse - Net Colon Plaque - Mucoid Plaquetigerlo75100% (1)
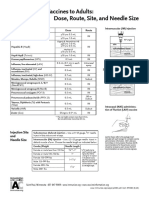
- Administering Vaccines To Adults: Dose, Route, Site, and Needle SizeDocument1 paginăAdministering Vaccines To Adults: Dose, Route, Site, and Needle SizeAkashÎncă nu există evaluări
- Designed To Move Full ReportDocument142 paginiDesigned To Move Full ReportAktibiliÎncă nu există evaluări
- Diagnostic Accuracy of Chest X-Ray for Interstitial Lung DiseaseDocument6 paginiDiagnostic Accuracy of Chest X-Ray for Interstitial Lung DiseaseShahid HussainÎncă nu există evaluări
- Khiveh 2017Document8 paginiKhiveh 2017Siti lestarinurhamidahÎncă nu există evaluări
- Augmentinsyr PDFDocument4 paginiAugmentinsyr PDFFiifi Andoh-kumiÎncă nu există evaluări
- Diabetes INSIPIDUSDocument6 paginiDiabetes INSIPIDUSavinash dhameriya100% (1)
- Physio Ex 8.0 Exercise 7 WorksheetDocument11 paginiPhysio Ex 8.0 Exercise 7 WorksheetCDN50% (2)
- PsyciaDocument6 paginiPsyciagunn twothingÎncă nu există evaluări
- Allergy Testing PDFDocument25 paginiAllergy Testing PDFRK MalhotraÎncă nu există evaluări
- CDC Guidelines For Isolation Precautions in HospitalsDocument5 paginiCDC Guidelines For Isolation Precautions in HospitalsReamonn Vincent DantesÎncă nu există evaluări
- Jurnal PsikiatriDocument4 paginiJurnal PsikiatriSri SiswatiÎncă nu există evaluări