S-ar putea să vă placă și
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Analysis of Cesarean Section Rate - According To Robson's 10-Group ClassificationDocument4 paginiAnalysis of Cesarean Section Rate - According To Robson's 10-Group ClassificationMahavir GemavatÎncă nu există evaluări
- 03 Humms 11 Pasay Stats and Prob s2 q1 w3Document20 pagini03 Humms 11 Pasay Stats and Prob s2 q1 w3Micashella ApanayÎncă nu există evaluări
- Dlmblse01-01 Course BookDocument116 paginiDlmblse01-01 Course BookGOPINATHÎncă nu există evaluări
- ACT PME Handbook - EnglishDocument92 paginiACT PME Handbook - EnglishNaveed UllahÎncă nu există evaluări
- Impact of E-Bills Payment On Customer Satisfaction in Uganda: Stanbic Bank Uganda Limited As The Case StudyDocument8 paginiImpact of E-Bills Payment On Customer Satisfaction in Uganda: Stanbic Bank Uganda Limited As The Case Study21-38010Încă nu există evaluări
- DDocument615 paginiDsimranÎncă nu există evaluări
- Synopsis by Deepanshi Shukla For Topic Cash Management at SBIDocument5 paginiSynopsis by Deepanshi Shukla For Topic Cash Management at SBIDeepanshi ShuklaÎncă nu există evaluări
- The Evolution of Tooth Wear Indices: ReviewDocument5 paginiThe Evolution of Tooth Wear Indices: ReviewBenjiÎncă nu există evaluări
- Historical Context of The Emergence of Each DisciplinesDocument43 paginiHistorical Context of The Emergence of Each DisciplinesBloodmier GabrielÎncă nu există evaluări
- Study of Service Quality Management in Hotel IndustryDocument5 paginiStudy of Service Quality Management in Hotel IndustryVuong Nguyen AnÎncă nu există evaluări
- Ey The Indian Organic Market Report Online Version 21 March 2018Document52 paginiEy The Indian Organic Market Report Online Version 21 March 2018Kamalaganesh Thirumeni100% (2)
- PBB in MauritiusDocument7 paginiPBB in MauritiusnewmadproÎncă nu există evaluări
- Winning The Zero Moment of Thruth With Marketing AutomationDocument28 paginiWinning The Zero Moment of Thruth With Marketing AutomationtinalaurenaÎncă nu există evaluări
- Cross-Readings of Schoenberg S SketchesDocument14 paginiCross-Readings of Schoenberg S SketchesStefanoÎncă nu există evaluări
- Behavior Prediction Through Handwriting Analysis: Parmeet Kaur Grewal, Deepak PrasharDocument4 paginiBehavior Prediction Through Handwriting Analysis: Parmeet Kaur Grewal, Deepak PrasharqwerÎncă nu există evaluări
- A Systematic Inventory of Motives For Becoming An Orchestra ConductorDocument17 paginiA Systematic Inventory of Motives For Becoming An Orchestra ConductorMirelaAlexandraÎncă nu există evaluări
- Structural Stigma and Its Impact On Healthcare For Borderline Personality Disorder: A Scoping ReviewDocument41 paginiStructural Stigma and Its Impact On Healthcare For Borderline Personality Disorder: A Scoping Reviewconsulta.nicolaslabbeÎncă nu există evaluări
- ECCU 500 Course SyllabusDocument14 paginiECCU 500 Course Syllabusrandom8000Încă nu există evaluări
- Child SocialLeadershipQualitiesDocument25 paginiChild SocialLeadershipQualitiesVincent FordÎncă nu există evaluări
- Personal Development PlanningDocument5 paginiPersonal Development Planningnandani20Încă nu există evaluări
- ThesisDocument64 paginiThesisiojnilnjkhÎncă nu există evaluări
- Intentional IgnoranceDocument41 paginiIntentional IgnoranceCat SkullÎncă nu există evaluări
- Two Sample Inference: By: Girma MDocument33 paginiTwo Sample Inference: By: Girma MAdinaan ShaafiiÎncă nu există evaluări
- General Introduction To Airborne Magnetic Survey PDFDocument15 paginiGeneral Introduction To Airborne Magnetic Survey PDFMithunÎncă nu există evaluări
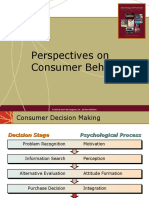
- Perspectives On Consumer Behavior: © 2003 Mcgraw-Hill Companies, Inc., Mcgraw-Hill/IrwinDocument28 paginiPerspectives On Consumer Behavior: © 2003 Mcgraw-Hill Companies, Inc., Mcgraw-Hill/IrwinUMAR KHANÎncă nu există evaluări
- Lecture in EntrepreneurshipDocument7 paginiLecture in EntrepreneurshipAnonymous xl2Fs9R8wÎncă nu există evaluări
- CV - Dr. DeLessio-ParsonDocument7 paginiCV - Dr. DeLessio-ParsonAx DeLessio-Parson, PhDÎncă nu există evaluări
- A Short Survey On The Usage of Choquet Integral and Its Associated Fuzzy Measure in Multiple Attribute AnalysisDocument8 paginiA Short Survey On The Usage of Choquet Integral and Its Associated Fuzzy Measure in Multiple Attribute AnalysisfarisÎncă nu există evaluări
- Chapter 3. Sales & Operations Aggregate) PlanningDocument47 paginiChapter 3. Sales & Operations Aggregate) PlanningsanjaykhatwaniÎncă nu există evaluări
- Chapter 5 Full SolutionsDocument21 paginiChapter 5 Full SolutionsBar AzilaÎncă nu există evaluări