S-ar putea să vă placă și
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- MLN CatalogDocument24 paginiMLN CatalogLhingboi100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Biology Questions and AnswersDocument472 paginiBiology Questions and Answersbusybeefreedom100% (1)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Schizophrenia and Biblical Counseling Notes Doc-DrDocument4 paginiSchizophrenia and Biblical Counseling Notes Doc-DrJulio Cezar de Pinho Jr.Încă nu există evaluări
- Tasha's Gynae Case WriteDocument6 paginiTasha's Gynae Case WriteMelissa Aina Mohd YusofÎncă nu există evaluări
- Everything About DogsDocument326 paginiEverything About Dogstobiasaxo5653100% (1)
- Drug Study Nov. 12Document6 paginiDrug Study Nov. 12Jenny Ajoc100% (4)
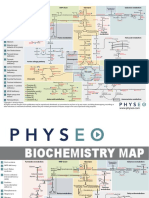
- 6 Biochemistry Map PDFDocument2 pagini6 Biochemistry Map PDFDipesh ShresthaÎncă nu există evaluări
- Introduction Integrative MedicineDocument13 paginiIntroduction Integrative MedicineNitin PatilÎncă nu există evaluări
- Asthma PhenotypesDocument55 paginiAsthma PhenotypesAnonymous so6ZnlKywÎncă nu există evaluări
- Picture a den full ofbaby deer (dendrites) receivingsignals from their mother.Soma: cell body of the neuronDocument36 paginiPicture a den full ofbaby deer (dendrites) receivingsignals from their mother.Soma: cell body of the neuronLouie OkayÎncă nu există evaluări
- Mefenamic AcidDocument2 paginiMefenamic AcidXtinego100% (1)
- Persona Knee Surgical TechniqueDocument72 paginiPersona Knee Surgical TechniquedrorthokingÎncă nu există evaluări
- Esthetic Inlays & OnlaysDocument32 paginiEsthetic Inlays & OnlaysYousif Abdulla75% (4)
- Common Sense On Mutual Funds 2Document1 paginăCommon Sense On Mutual Funds 2Dipesh ShresthaÎncă nu există evaluări
- Obstetric Hemorrhage AnestDocument9 paginiObstetric Hemorrhage AnestjefeÎncă nu există evaluări
- BPKIHSDocument38 paginiBPKIHSDipesh ShresthaÎncă nu există evaluări
- Clincal Sciences Major R..Document6 paginiClincal Sciences Major R..Dipesh ShresthaÎncă nu există evaluări
- Management of Obstetric Haemorrhage 3 1Document8 paginiManagement of Obstetric Haemorrhage 3 1Dipesh Shrestha100% (1)
- CHS MCQ Self AssessmentDocument7 paginiCHS MCQ Self AssessmentDipesh ShresthaÎncă nu există evaluări
- Moles, Osmoles, and Movement - Fact Sheet - 0Document7 paginiMoles, Osmoles, and Movement - Fact Sheet - 0Dipesh ShresthaÎncă nu există evaluări
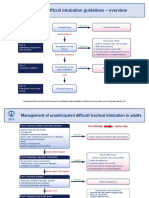
- Difficult Intubation Guidelines OverviewDocument3 paginiDifficult Intubation Guidelines OverviewMaufer AlÎncă nu există evaluări
- Lactate FaqDocument4 paginiLactate FaqMuhammad RizqiÎncă nu există evaluări
- Modifying Ventilator Settings Based On The PaCO2Document1 paginăModifying Ventilator Settings Based On The PaCO2Dipesh ShresthaÎncă nu există evaluări
- IBE II MCQ Questions 4th BatchDocument18 paginiIBE II MCQ Questions 4th BatchDipesh ShresthaÎncă nu există evaluări
- The What and Why of Mechanical VentilationDocument1 paginăThe What and Why of Mechanical VentilationDipesh ShresthaÎncă nu există evaluări
- SJT 2Document64 paginiSJT 2Dipesh ShresthaÎncă nu există evaluări
- Clinical Sciences Medicine Self AssessmentDocument6 paginiClinical Sciences Medicine Self AssessmentDipesh ShresthaÎncă nu există evaluări
- Tokyo Guidelines 2018 Flowchart For The ManagementDocument19 paginiTokyo Guidelines 2018 Flowchart For The ManagementDipesh ShresthaÎncă nu există evaluări
- Annals of Surgery Volume Issue 2018Document8 paginiAnnals of Surgery Volume Issue 2018Dipesh ShresthaÎncă nu există evaluări
- SJT 1Document64 paginiSJT 1Dipesh ShresthaÎncă nu există evaluări
- 2015 AHA CPR & ECC Guidelines AlgorithmsDocument20 pagini2015 AHA CPR & ECC Guidelines AlgorithmsDipesh Shrestha100% (1)
- 10 1001@jama 2016 0287Document10 pagini10 1001@jama 2016 0287ompardor7554Încă nu există evaluări
- Biology Syllabus HSEBDocument2 paginiBiology Syllabus HSEBDipesh ShresthaÎncă nu există evaluări
- ACG Guideline AcutePancreatitis September 2013Document16 paginiACG Guideline AcutePancreatitis September 2013gorditomaloÎncă nu există evaluări
- Surgical Safety ChecklistDocument1 paginăSurgical Safety Checklistmillechilli1Încă nu există evaluări
- Drug of ChoiceDocument3 paginiDrug of ChoiceDipesh ShresthaÎncă nu există evaluări
- 7690-3638 High School Science Biology Student Resource Book 08-09 PDFDocument240 pagini7690-3638 High School Science Biology Student Resource Book 08-09 PDFGustavo KstÎncă nu există evaluări
- Biology Syllabus HSEBDocument2 paginiBiology Syllabus HSEBDipesh ShresthaÎncă nu există evaluări
- Vechur Cattle Breed Questions and AnswersDocument39 paginiVechur Cattle Breed Questions and AnswersvgasÎncă nu există evaluări
- Note By4 By5Document263 paginiNote By4 By5Ae BanpongÎncă nu există evaluări
- Testing Anxiety in Undergraduate Medical Students and Its Correlation With Different Learning ApproachesDocument11 paginiTesting Anxiety in Undergraduate Medical Students and Its Correlation With Different Learning ApproachesJosé Carlos Sánchez-RamirezÎncă nu există evaluări
- Diabetic Ketoacidosis Protocol PICU Oct 2010 2Document9 paginiDiabetic Ketoacidosis Protocol PICU Oct 2010 2Vidini Kusuma AjiÎncă nu există evaluări
- Diverticulosis!!Document10 paginiDiverticulosis!!Nahdah AidahÎncă nu există evaluări
- Massive Transfusion Complications: Citrate Toxicity, Coagulopathy, Electrolyte ImbalancesDocument1 paginăMassive Transfusion Complications: Citrate Toxicity, Coagulopathy, Electrolyte ImbalancesDennis Nabor Muñoz, RN,RMÎncă nu există evaluări
- FERRIC CARBOXYMALTOSE IMPROVES SYMPTOMS IN HEART FAILURE PATIENTS WITH IRON DEFICIENCYDocument31 paginiFERRIC CARBOXYMALTOSE IMPROVES SYMPTOMS IN HEART FAILURE PATIENTS WITH IRON DEFICIENCYDanar Fahmi SudarsonoÎncă nu există evaluări
- Research Revision Version 10 (Clean Copy)Document27 paginiResearch Revision Version 10 (Clean Copy)Nesty Perez IIIÎncă nu există evaluări
- Foreign and Local Literature Fatigue Among NursesDocument5 paginiForeign and Local Literature Fatigue Among NursesMay Therese B. BoriborÎncă nu există evaluări
- Dental Implant Awareness Among Patients in Our Institution in Chennai-Cross-Sectional SurveyDocument4 paginiDental Implant Awareness Among Patients in Our Institution in Chennai-Cross-Sectional SurveyInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- VijayDocument12 paginiVijaykishanÎncă nu există evaluări
- Voluntary Rehab DOHDocument15 paginiVoluntary Rehab DOHFebiana Bayacsan100% (1)
- Resp TestDocument7 paginiResp TestKong KongÎncă nu există evaluări
- FUROSEMIDEDocument2 paginiFUROSEMIDEjbespiritu100% (3)
- HAAD-Policy Scope of Practice For Practical Nurse PDFDocument4 paginiHAAD-Policy Scope of Practice For Practical Nurse PDFmyangel_peach3305Încă nu există evaluări
- B20 Patient Monitor BrochureDocument6 paginiB20 Patient Monitor Brochurehphphp00Încă nu există evaluări
- Hyperkalemia Approach AND Management: Dr. Renuka RayanaDocument38 paginiHyperkalemia Approach AND Management: Dr. Renuka RayanaSap ModulesÎncă nu există evaluări
- HR 1701 - Commending Medical and Nursing Board TopnotchersDocument2 paginiHR 1701 - Commending Medical and Nursing Board TopnotchersBayan Muna Party-listÎncă nu există evaluări
- Topic 1 What Is Patient Safety?Document14 paginiTopic 1 What Is Patient Safety?Lilik WijayatiÎncă nu există evaluări
- Resume Only 2018Document2 paginiResume Only 2018api-430903191Încă nu există evaluări
- TB Screening in Pregnancy 1Document32 paginiTB Screening in Pregnancy 1nurfitriwidiÎncă nu există evaluări
- Dagupan University drug study templateDocument4 paginiDagupan University drug study templateKhatlene Joy RaymundoÎncă nu există evaluări