S-ar putea să vă placă și
- CBSE Parent Consent Form PDFDocument2 paginiCBSE Parent Consent Form PDFVivekÎncă nu există evaluări
- Adjusting Entries: Date Doc. No. Description REF Debet CreditDocument11 paginiAdjusting Entries: Date Doc. No. Description REF Debet CreditEka WiraÎncă nu există evaluări
- Click! Game OverDocument49 paginiClick! Game Overekoga_emeriÎncă nu există evaluări
- 37ladera3 Gasset 72Document1 pagină37ladera3 Gasset 72Jubayer SabujÎncă nu există evaluări
- Moon Journal PDFDocument1 paginăMoon Journal PDFAlbertGyörgynéFeketeJudit100% (1)
- Ukelele 3.5 TutorialDocument62 paginiUkelele 3.5 TutorialCláudioÎncă nu există evaluări
- Design SheetDocument1 paginăDesign SheetBrian LuisÎncă nu există evaluări
- Date Work Summary/Weekly Activities Duration Remarks: Log BookDocument24 paginiDate Work Summary/Weekly Activities Duration Remarks: Log BookShalini NishaÎncă nu există evaluări
- Metatronic Bible v5 - Metatron ArchangelDocument4.398 paginiMetatronic Bible v5 - Metatron ArchangelTony YusteinÎncă nu există evaluări
- Arasco Induction 3 NewDocument20 paginiArasco Induction 3 NewSyed Nazar AlamÎncă nu există evaluări
- Chiller York San Lorenzo Ycal0024Document112 paginiChiller York San Lorenzo Ycal0024fishy254Încă nu există evaluări
- Ingalls Classroom Mangement PlanDocument7 paginiIngalls Classroom Mangement Planapi-568146761Încă nu există evaluări
- Psy 2 - AbpsyDocument13 paginiPsy 2 - AbpsyYDEL MIKAELA CABALANG TIBONÎncă nu există evaluări
- Vaccination RecordDocument2 paginiVaccination RecordThembaÎncă nu există evaluări
- Stren Exer Ngth/weigh Rcise HTS: Sets # Weight R Reps Wei Ight Reps Weight Reps Wei Ight RepsDocument1 paginăStren Exer Ngth/weigh Rcise HTS: Sets # Weight R Reps Wei Ight Reps Weight Reps Wei Ight RepsPhong LeÎncă nu există evaluări
- Nets For Making Solids UDocument8 paginiNets For Making Solids ULuis Javier RodriguezÎncă nu există evaluări
- I'M STILL HEALING: A poetry collection of love and trauma.De la EverandI'M STILL HEALING: A poetry collection of love and trauma.Încă nu există evaluări
- 3 Pengukuran Sipat Datar Memanjang Pergi Pulang Dan Profil Melintang 2Document28 pagini3 Pengukuran Sipat Datar Memanjang Pergi Pulang Dan Profil Melintang 2sehastra100% (1)
- 3.transport Allce Cert (Version 1Document1 pagină3.transport Allce Cert (Version 1Tushar ChaudharyÎncă nu există evaluări
- Dixon Kodiak Series 2008-2009 Parts ManualDocument40 paginiDixon Kodiak Series 2008-2009 Parts ManualPaul AllansonÎncă nu există evaluări
- PerceptronSVM Module5 Part2 October2023Document43 paginiPerceptronSVM Module5 Part2 October2023Sarwan ShahÎncă nu există evaluări
- Mazahib Ka Taqabuli Jayiza Asal PDFDocument58 paginiMazahib Ka Taqabuli Jayiza Asal PDFShaikhÎncă nu există evaluări
- Rave New Year 2021 Forecast - EbookDocument38 paginiRave New Year 2021 Forecast - EbookFiona Huang100% (2)
- Floorplan - Exhibit Hall Ai4 2022 - Booth SelectionDocument1 paginăFloorplan - Exhibit Hall Ai4 2022 - Booth SelectionPriya RanaÎncă nu există evaluări
- Generator Load Recording SheetDocument1 paginăGenerator Load Recording SheetArturo Ramos Alvezo100% (2)
- Letter of IntentDocument1 paginăLetter of IntentCath DiÎncă nu există evaluări
- Survey Plans KIKOMBO DODOMADocument1 paginăSurvey Plans KIKOMBO DODOMAJin LìÎncă nu există evaluări
- Anita La Bogotana. Partitura PDFDocument4 paginiAnita La Bogotana. Partitura PDFSebastian Escobar CaroÎncă nu există evaluări
- Anita La Bogotana. Partitura PDFDocument4 paginiAnita La Bogotana. Partitura PDFPaulo Cesar Osorio CabreraÎncă nu există evaluări
- 1ESO - Tema 4Document4 pagini1ESO - Tema 4mintoterÎncă nu există evaluări
- Https Woqode - Com CR S 2520&r 302911405Document1 paginăHttps Woqode - Com CR S 2520&r 302911405RòsèAñ KcÎncă nu există evaluări
- V320BJ7 Pe1 InnoluxDocument33 paginiV320BJ7 Pe1 InnoluxLuis LeónÎncă nu există evaluări
- S1 Maths 2018-19 - CE-1 PDFDocument2 paginiS1 Maths 2018-19 - CE-1 PDFFredy F RÎncă nu există evaluări
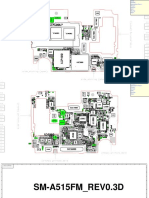
- SM-A515FM REV0.3D SCH PCBDocument12 paginiSM-A515FM REV0.3D SCH PCBiRem MasterÎncă nu există evaluări
- Capacity Charts For The FT14, FT14HC, FTGS14 and FTGS14HC Ball Float Steam Traps at Low Differential PressureDocument2 paginiCapacity Charts For The FT14, FT14HC, FTGS14 and FTGS14HC Ball Float Steam Traps at Low Differential PressureErce KoyunbabaÎncă nu există evaluări
- 由布列茲《訊息速寫》之分析至自身音樂創作的應用 PDFDocument105 pagini由布列茲《訊息速寫》之分析至自身音樂創作的應用 PDFShi-Lin HongÎncă nu există evaluări
- Viven Aparentando - Trumpet in BB 1Document2 paginiViven Aparentando - Trumpet in BB 1Daniel GarciaÎncă nu există evaluări
- Summer Training ContentDocument3 paginiSummer Training ContentvinayÎncă nu există evaluări
- Spmed Timesheet 2Document1 paginăSpmed Timesheet 2api-340778375Încă nu există evaluări
- Spmed Timesheet 2Document1 paginăSpmed Timesheet 2api-355830788Încă nu există evaluări
- Spmed Timesheet Second SemesterDocument1 paginăSpmed Timesheet Second Semesterapi-340688414Încă nu există evaluări
- Air-Cooled Scroll Chillers: Style DDocument80 paginiAir-Cooled Scroll Chillers: Style Djuan beltranÎncă nu există evaluări
- ACT ScantronDocument2 paginiACT ScantronnonsenseÎncă nu există evaluări
- ACT ScantronDocument2 paginiACT ScantronnonsenseÎncă nu există evaluări
- ACT ScantronDocument2 paginiACT ScantronnonsenseÎncă nu există evaluări
- Havij 1.15 Pro by R3Dm0V3: Targ Et: Date: 16/04/2019 09:50:47 DB Dete Ction: Mysql (Auto Detected)Document29 paginiHavij 1.15 Pro by R3Dm0V3: Targ Et: Date: 16/04/2019 09:50:47 DB Dete Ction: Mysql (Auto Detected)Bianca SiqueiraÎncă nu există evaluări
- Revision Table: Afcons Infrastructure LimitedDocument16 paginiRevision Table: Afcons Infrastructure LimitedSarbajit Roy ChoudhuryÎncă nu există evaluări
- Michael Graham LawsuitDocument23 paginiMichael Graham LawsuitThe Kansas City StarÎncă nu există evaluări
- Book Sale Volunteer ApplicationDocument2 paginiBook Sale Volunteer Applicationlaurabrown63Încă nu există evaluări
- Basement Plan: Proposed Villa B+G+1+Ph+ Swimming Pool + Ancillary BlocksDocument1 paginăBasement Plan: Proposed Villa B+G+1+Ph+ Swimming Pool + Ancillary BlocksNAHEEMA KPÎncă nu există evaluări
- Report On Voters With Incorrect Data in The VrridDocument1 paginăReport On Voters With Incorrect Data in The Vrrideric austriaÎncă nu există evaluări
- 2010 Trenier BroadwayDocument6 pagini2010 Trenier BroadwayBetoguitar777Încă nu există evaluări
- Stella by Starlight: Ron CarterDocument4 paginiStella by Starlight: Ron CarterMPÎncă nu există evaluări
- ISOMETRIADocument1 paginăISOMETRIAacsproyectos10Încă nu există evaluări
- Disney Themes - The Bear NecessitiesDocument1 paginăDisney Themes - The Bear NecessitiesАрсен ХизриевÎncă nu există evaluări
- Last Name First Name Middle Name Address Contact NoDocument2 paginiLast Name First Name Middle Name Address Contact NoGerome Bautista VInluanÎncă nu există evaluări
- ME Quest of The RIngbearer 2020 PREVIEWDocument8 paginiME Quest of The RIngbearer 2020 PREVIEWTpTVelem0% (2)
- White Shade: The Real-World Primer for the Black Professional WomanDe la EverandWhite Shade: The Real-World Primer for the Black Professional WomanÎncă nu există evaluări
- Adult Critical Care IV Medication Infusion Sheet PDFDocument2 paginiAdult Critical Care IV Medication Infusion Sheet PDFihtisham1Încă nu există evaluări
- Epidural Dosing ChartDocument1 paginăEpidural Dosing Chartihtisham1Încă nu există evaluări
- Anaesthesia Notes Sudan PDFDocument1 paginăAnaesthesia Notes Sudan PDFihtisham1Încă nu există evaluări
- SAVE That Line!Document5 paginiSAVE That Line!ihtisham1Încă nu există evaluări
- Azkar After Farz PrayerDocument16 paginiAzkar After Farz Prayerihtisham1Încă nu există evaluări
- Anaesthesia Notes Sudan PDFDocument1 paginăAnaesthesia Notes Sudan PDFihtisham1Încă nu există evaluări
- Allama Iqbal Aur Hum DR Israr AhmadDocument128 paginiAllama Iqbal Aur Hum DR Israr AhmadUrdu_LiteratureÎncă nu există evaluări
- 2 Drugs For General AnaesthesiaDocument27 pagini2 Drugs For General Anaesthesiaihtisham1Încă nu există evaluări
- Standard Operating Procedure : Anaesthesia DepartmentDocument3 paginiStandard Operating Procedure : Anaesthesia Departmentihtisham1Încă nu există evaluări
- Management The Collapsed VictimDocument1 paginăManagement The Collapsed Victimihtisham1Încă nu există evaluări
- Airway AssessmentDocument24 paginiAirway AssessmentAbdul Hamid Alraiyes100% (1)
- Standard Operating Procedure : Anaesthesia DepartmentDocument3 paginiStandard Operating Procedure : Anaesthesia Departmentihtisham1Încă nu există evaluări
- Abcs LOC GCS Ringer's TKO: Diabetic Emergencies/Hyperglycemia (Ketoacidosis) Guidelines For CareDocument1 paginăAbcs LOC GCS Ringer's TKO: Diabetic Emergencies/Hyperglycemia (Ketoacidosis) Guidelines For Careihtisham1Încă nu există evaluări
- Protocol For SreptokinaseDocument1 paginăProtocol For Sreptokinaseihtisham1Încă nu există evaluări
- ANAPHYLAXIS GUIDELINESDocument1 paginăANAPHYLAXIS GUIDELINESihtisham1Încă nu există evaluări
- CVC Packs HornsbyDocument1 paginăCVC Packs Hornsbyihtisham1Încă nu există evaluări
- Standard Operating Procedure : Anaesthesia DepartmentDocument4 paginiStandard Operating Procedure : Anaesthesia Departmentihtisham1Încă nu există evaluări
- SRNA Orientation Checklist TitleDocument40 paginiSRNA Orientation Checklist Titleihtisham1Încă nu există evaluări
- Pop Ward ChecklistDocument6 paginiPop Ward Checklistihtisham1Încă nu există evaluări
- Quality of Handovers of Patients in Intensive Care UnitsDocument2 paginiQuality of Handovers of Patients in Intensive Care Unitsihtisham1Încă nu există evaluări
- NEWBORN RESUSCITATION PREPARATIONDocument2 paginiNEWBORN RESUSCITATION PREPARATIONihtisham1Încă nu există evaluări
- Prepation Surgery FormDocument1 paginăPrepation Surgery Formihtisham1Încă nu există evaluări
- Preop Checklist for Safe SurgeryDocument1 paginăPreop Checklist for Safe Surgeryihtisham1Încă nu există evaluări
- Investigation ChartDocument1 paginăInvestigation Chartihtisham1Încă nu există evaluări
- BASICS Newborn Resuscitation Learning GuideDocument3 paginiBASICS Newborn Resuscitation Learning Guideihtisham1Încă nu există evaluări
- Procedure PacksDocument1 paginăProcedure Packsihtisham1Încă nu există evaluări
- Post Operative Ward ChecklistsDocument4 paginiPost Operative Ward Checklistsihtisham1Încă nu există evaluări
- Disinf SterlizationDocument1 paginăDisinf Sterlizationihtisham1Încă nu există evaluări
- PAA Questionnaire ModifiedDocument1 paginăPAA Questionnaire Modifiedihtisham1Încă nu există evaluări
- Mahabharata Book 9 Shalya ParvaDocument413 paginiMahabharata Book 9 Shalya Parvaavacdis1969Încă nu există evaluări
- Socsci 032 Midterm Compilation NotesDocument12 paginiSocsci 032 Midterm Compilation NotesCarla AbalaÎncă nu există evaluări
- Academic StyleDocument4 paginiAcademic StyleHa ToÎncă nu există evaluări
- Past Paper 1 Ibsl: Phone: 7514251,0816930718Document4 paginiPast Paper 1 Ibsl: Phone: 7514251,0816930718santhiÎncă nu există evaluări
- Neural Networks in Data Mining: Ripundeep Singh Gill, AshimaDocument6 paginiNeural Networks in Data Mining: Ripundeep Singh Gill, AshimaIOSRJEN : hard copy, certificates, Call for Papers 2013, publishing of journalÎncă nu există evaluări
- 2.3 Temperature Conversions: Chapter 2 Energy and MatterDocument18 pagini2.3 Temperature Conversions: Chapter 2 Energy and MatterBeverly PamanÎncă nu există evaluări
- Gram Negative Rods NonStool Pathogens FlowchartDocument1 paginăGram Negative Rods NonStool Pathogens FlowchartKeithÎncă nu există evaluări
- Numerical Methods NotesDocument21 paginiNumerical Methods Notesdean427Încă nu există evaluări
- A P1qneer 1n Neuroscience: Rita Levi-MontalciniDocument43 paginiA P1qneer 1n Neuroscience: Rita Levi-MontalciniAntÎncă nu există evaluări
- Vaiana Et Al (2021)Document11 paginiVaiana Et Al (2021)Raffaele CapuanoÎncă nu există evaluări
- KoL Mekflu - 9Document104 paginiKoL Mekflu - 9Maha D NugrohoÎncă nu există evaluări
- Revit Mep Vs Autocad MepDocument4 paginiRevit Mep Vs Autocad MepAbdelhameed Tarig AlemairyÎncă nu există evaluări
- Contract Law 17Document1 paginăContract Law 17lorraineÎncă nu există evaluări
- Comparing Means of Two GroupsDocument8 paginiComparing Means of Two GroupsRobert Kier Tanquerido TomaroÎncă nu există evaluări
- 1) How Are Lakes Classified in Regards To Trophic Status? 2) What Is Cultural Eutrophication?Document31 pagini1) How Are Lakes Classified in Regards To Trophic Status? 2) What Is Cultural Eutrophication?Enzo TapingÎncă nu există evaluări
- UI Symphony Orchestra and Choirs Concert Features Mahler's ResurrectionDocument17 paginiUI Symphony Orchestra and Choirs Concert Features Mahler's ResurrectionJilly CookeÎncă nu există evaluări
- Lali The Sun Also Rises Final PaperDocument4 paginiLali The Sun Also Rises Final PaperDaniel AdamsÎncă nu există evaluări
- Durgah Ajmer Sharif 1961Document19 paginiDurgah Ajmer Sharif 1961Deepanshu JharkhandeÎncă nu există evaluări
- HazopDocument4 paginiHazopbaaziz2015Încă nu există evaluări
- Gee1-Lp1 2022-2023Document18 paginiGee1-Lp1 2022-2023Sherrizah AlidoÎncă nu există evaluări
- Checking battery control unitDocument3 paginiChecking battery control unitjuanÎncă nu există evaluări
- M and S - Capstone Marketing Across Cultures Fons TrompenaarsDocument398 paginiM and S - Capstone Marketing Across Cultures Fons TrompenaarsBof BeosÎncă nu există evaluări
- Thesis NewDocument55 paginiThesis NewHasan juwelÎncă nu există evaluări
- Lesson Plan For DemoDocument7 paginiLesson Plan For DemoShiela Tecson GamayonÎncă nu există evaluări
- Wag Acquisition v. Vubeology Et. Al.Document29 paginiWag Acquisition v. Vubeology Et. Al.Patent LitigationÎncă nu există evaluări
- IFU Egg Yolk Tellurite EmulsionDocument4 paginiIFU Egg Yolk Tellurite EmulsionoktaÎncă nu există evaluări
- Configuring Cisco Easy VPN and Easy VPN Server Using SDM: Ipsec VpnsDocument56 paginiConfiguring Cisco Easy VPN and Easy VPN Server Using SDM: Ipsec VpnsrajkumarlodhÎncă nu există evaluări
- Advanced Java Thread Lab ExercisesDocument9 paginiAdvanced Java Thread Lab ExercisesafalonsoÎncă nu există evaluări
- Useful List of Responsive Navigation and Menu Patterns - UI Patterns - GibbonDocument16 paginiUseful List of Responsive Navigation and Menu Patterns - UI Patterns - Gibbonevandrix0% (1)
- Lab ReportDocument11 paginiLab Reportkelvinkiplaa845Încă nu există evaluări